
Журнал «Медицина неотложных состояний» Том 22, №3, 2026
Вернуться к номеру
Шкала MMSE в діагностиці когнітивної дисфункції у пацієнтів після ендопротезування кульшового суглоба під спінальною анестезією
Авторы: Дацюк О.І. (1, 2), Свіргун М.В. (3), Гончарук О.С. (2), Дацюк Л.В. (4), Куцик О.В. (2, 5), Бевз Г.В. (1, 2), Пашинський Я.М. (1, 2), Козловський Ю.К. (2), Дмитришин С.П. (1, 2), Козловська І.Ю. (2), Балацький О.Р. (2), Вознюк Т.О. (1, 2), Дмитрієва Е.М. (1, 2), Озимий В.А. (6)
(1) - Вінницька обласна клінічна лікарня імені М.І. Пирогова, м. Вінниця, Україна
(2) - Вінницький національний медичний університет імені М.І. Пирогова, м. Вінниця, Україна
(3) - ТОВ «Інномед — Материнство та дитинство», м. Вінниця, Україна
(4) - Подільський регіональний центр онкології, м. Вінниця, Україна
(5) - Вінницька міська клінічна лікарня швидкої медичної допомоги, м. Вінниця, Україна
(6) - Військова частина А1065, 409 військовий госпіталь, м. Житомир, Україна
Рубрики: Медицина неотложных состояний
Разделы: Клинические исследования
Версия для печати
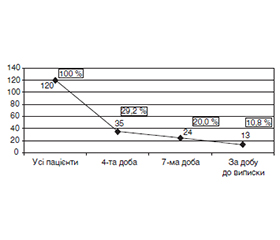
Актуальність. Післяопераційні когнітивні розлади є предиктором розвитку стійкої когнітивної дисфункції й підвищують ризик розвитку деменції. Протягом останніх двох десятиліть спостерігається зростання числа ортопедичних утручань, виконаних в умовах спінальної анестезії, з приводу гострої травми чи дегенеративної суглобової патології. Виникнення когнітивного дефіциту в ранньому післяопераційному періоді в осіб похилого віку є доведеним фактом. Проблема аналізу діагностичних критеріїв та адекватної нейропротекторної корекції післяопераційної когнітивної дисфункції (ПОКД) при ендопротезуванні кульшового суглоба залишається не вирішеною повною мірою. Мета: вивчення негативної динаміки когнітивних функцій на різних строках після ендопротезування кульшового суглоба під спінальною анестезією. Матеріали та методи. Кількість хворих, які були включені в дослідження — 120. Усі хворі лікувалися в травматологічному відділенні КНП «Вінницька міська клінічна лікарня швидкої медичної допомоги». Як одну з основних оціночних шкал ПОКД використовували шкалу Mini-Mental State Examination (MMSE). Нейрокогнітивне тестування для визначення стану вищої нервової дiяльностi проводили за добу до операції, повторну оцінку здійснювали на 4-ту та 7-му добу після операції та за добу до виписки зі стаціонару. Статистичну обробку даних проводили з використанням можливостей електронних таблиць Microsoft Excel і пакета статистичної обробки інформації SPSS 23.0. Результати. У переважної (77,1 %) більшості пацієнтів на 4-ту добу після ендопротезування кульшового суглоба негативна динаміка когнітивної функції проявлялась у вигляді появи легких когнітивних розладів при їх відсутності та появи когнітивних порушень рівня деменції середнього ступеня тяжкості при наявності їх легкого ступеня на момент госпіталізації пацієнтів. На 7-му добу проти 4-ї доби реєструється зменшення випадків зміни когнітивного статусу порівняно з показниками на момент госпіталізації. І за добу до виписки лише в 13 із 35 осіб (37,1 %) зберігалась негативна динаміка когнітивної функції, від загальної вибірки частка цих пацієнтів становила майже 11 %. Висновки. На підставі проведеного аналізу даних про стан змін когнітивної функції в післяопераційному періоді порівняно з доопераційним станом автори дійшли висновку, що шкала MMSE в періопераційному періоді може бути використана для діагностики когнітивних порушень та як критерій ефективності корекції когнітивних порушень у таких хворих з метою проведення подальшої терапії.
Background. Postoperative cognitive impairment is a predictor of persistent cognitive dysfunction and increases the risk of dementia. Over the past two decades, there has been an increase in the number of orthopedic procedures performed under spinal anesthesia for acute trauma or degenerative joint disease. The occurrence of cognitive deficits in the early postoperative period in the elderly is a proven fact. The problem of analyzing diagnostic criteria and adequate neuroprotective correction of postoperative cognitive dysfunction in hip arthroplasty remains not fully resolved. Purpose: to study the negative dynamics of cognitive functions at different times after hip arthroplasty under spinal anesthesia. Materials and methods. The number of patients included in the study was 120. All participants were treated at the trauma unit of the Vinnytsia City Clinical Emergency Hospital. The Mini-Mental State Examination (MMSE) was used as one of the main assessment scales in postoperative cognitive dysfunction. Neurocognitive testing to determine the state of higher nervous activity was performed the day before operation, repeated assessment was carried out on the 4th and 7th days after surgery, and the day before discharge from the hospital. Statistical data processing was performed using the capabilities of spreadsheets of Microsoft Excel and the statistical information processing package SPSS 23.0. Results. In the vast majority (77.1 %) of patients on the 4th day after hip arthroplasty, the negative dynamics of cognitive function was manifested in the form of the appearance of mild cognitive impairment with their absence at the time of hospitalization and the appearance of cognitive disorders of moderate dementia level in the presence of their mild degree at the time of hospitalization. On the 7th day versus the 4th day, a decrease in cases of change in cognitive status is recorded compared to the indicators at the time of hospitalization. And the day before discharge, only 13 out of 35 (37.1 %) cases had negative dynamics of cognitive function; from the total sample, the share of these patients was almost 11 %. Conclusions. Based on the analysis of data on the state of changes in cognitive function, when comparing the postoperative period with the preoperative state, the MMSE in the perioperative period can be used to diagnose cognitive disorders and as a criterion for the effectiveness of correction of cognitive impairment in these patients for the purpose of further therapy.
хірургічне втручання; спінальна анестезія, ендопротезування кульшового суглоба; MMSE; когнітивні функції; нейропсихологічний дефіцит
surgery; spinal anesthesia; hip replacement; Mini-Mental State Examination; cognitive functions; neuropsychological deficit