
Журнал «Медицина неотложных состояний» Том 22, №3, 2026
Вернуться к номеру
Генералізована безеритемна форма системного кліщового бореліозу: труднощі діагностики (клінічний випадок)
Авторы: Міщенко В.А. (1), Одинець І.Ю. (1), Пушкар М.Б. (1), Ольховська О.М. (1), Гриньов Р.М. (2), Желєзнікова М.О. (1), Малоштан В.А. (1)
(1) - Харківський національний медичний університет, м. Харків, Україна
(2) - Харківський національний університет імені В.Н. Каразіна, м. Харків, Україна
Рубрики: Медицина неотложных состояний
Разделы: Справочник специалиста
Версия для печати
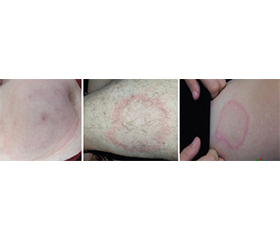
Безеритемні форми хвороби Лайма — системного кліщового бореліозу (СКБ) вважаються одними з найскладніших для діагностики через відсутність патогномонічного (специфічного) маркера захворювання — мігруючої еритеми. У такій ситуації клініцисту слід враховувати сезон, проживання чи перебування хворого в ендемічному щодо СКБ регіоні, можливість реалізації аліментарного шляху інфікування бореліями при вживанні молочних продуктів від хворих домашніх тварин. Безеритемна форма СКБ часто перебігає як звичайне ГРВІ або грип та починається з гарячки, слабкості, головного болю, болю у м’язах та суглобах. Іноді хвороба маскується під інші патології: міокардит, хоріоретиніт, неврологічні розлади (параліч лицьового нерва, радикулопатії, менінгоенцефаліт), гепатит. Поява у хворого в ендемічному щодо активності кліщів регіоні будь-якої симптоматики без мігруючої еритеми потребує обстеження на СКБ, якщо ця симптоматика не пояснюється іншими нозологічними формами. З метою виявлення специфічних титрів антитіл та оцінки їх динаміки призначають серологічне тестування крові методом ІФА та повторне — через 2–4 тижні. Діагностично значущим є дослідження ліквору методом ПЛР на наявність борелій при менінгоенцефалітах. Недооцінка вищезазначених клініко-анамнестичних даних та лабораторних критеріїв призводить до помилкового діагнозу, несвоєчасного призначення лікування та значно підвищує ризик розвитку хронічних форм захворювання та ускладнень.
Non-erythematous forms of systemic tick-borne borreliosis, or Lyme disease (LD), are considered one of the most difficult to diagnose due to the lack of a pathognomonic (specific) marker of the disease — erythema migrans. In such a situation, the clinician should take into account the season, the patient’s residence or stay in a region endemic for LD, the possibility of an alimentary route of infection with Borrelia when consuming dairy products from sick domestic animals. The non-erythematous form of LD often proceeds as a common acute respiratory viral infection or flu and begins with the appearance of fever, weakness, headache, pain in muscles and joints. Sometimes the disease is masked as other pathologies: myocarditis, chorioretinitis, neurological disorders (facial nerve palsy, radiculopathy, meningoencephalitis), hepatitis. The appearance in a patient in a region endemic for tick activity of any symptoms without erythema migrans requires examination for LD, if these symptoms are not explained by other nosological forms. In order to identify specific antibody titers and assess their dynamics, serological blood testing is prescribed by the enzyme-linked immunosorbent assay, with a repeat after 2–4 weeks. The study of cerebrospinal fluid by polymerase chain reaction for the presence of Borrelia is diagnostically significant in cases of meningoencephalitis. Underestimation of the above-mentioned clinical and anamnestic data and laboratory criteria leads to diagnostic errors, delayed treatment and significantly increases the risk of developing chronic forms of the disease and complications.
системний кліщовий бореліоз; хвороба Лайма; безеритемна форма; клініка; діагностика
systemic tick-borne borreliosis; Lyme disease; non-erythematous form; clinical features; diagnosis
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Esposito S., Bosis S., Sabatini C. et al. Borrelia burgdorferi infection and Lyme disease in children. Int J Infect Dis. 2013 Mar;17(3):e153-8. doi: 10.1016/j.ijid.2012.09.014.
- Shapiro E.D. Borrelia burgdorferi (Lyme disease). Pediatr Rev. 2014 Dec;35(12):500-9. doi: 10.1542/pir.35-12-500.
- Steere A.C., Strle F., Wormser G.P. et al. Lyme borreliosis. Nat Rev Dis Primers. 2016 Dec 15;2:16090. doi: 10.1038/nrdp.2016.90.
- Trevisan G., Bonin S., Ruscio M. A Practical Approach to the Diagnosis of Lyme Borreliosis: From Clinical Heterogeneity to Laboratory Methods. Front Med (Lausanne). 2020 Jul 23;7:265. doi: 10.3389/fmed.2020.00265.
- Greiter B.M., Sidorov S., Osuna E. et al. Clinical characte–ristics and serological profiles of Lyme disease in children: a 15-year retrospective cohort study in Switzerland. Lancet Reg Health Eur. 2024 Dec 9;48:101143. doi: 10.1016/j.lanepe.2024.101143.
- Nadraga O.B., Dybas I.V., Hladchenko O.I. et al. Neuroborreliosis in children: report of case and a review of the literature. Problems of Clinical Pediatrics. 2023;3(61):64-67. doi: 10.24144/1998-6475.2023.61.64-67.
- McCarthy C.A., Helis J.A., Daikh B.E. Lyme Disease in Children. Infect Dis Clin North Am. 2022 Sep;36(3):593-603. doi: 10.1016/j.idc.2022.03.002.
- Zhuk O.O., Shkilna M.I. Liver damage in patients with Lyme borreliosis with skin damage (multiple erythema migrans). Prospects and innovations of science. 2024;20(44):1317-1324. doi: 10.52058/2786-4952-2024-10(44)-1317-1324 (In Ukrainian).
- Lytvyn H.O., Basa N.R. Laboratory characterisics of erythemous and non-erythemous forms of Lyme disease in children. Actual Problems of Pediatrics, Obstetrics and Gynecology. 2024;2:41-48. doi: 10.11603/24116-4944.2023.2.14259 (In Ukrainian).
- Semchyshyn I.A., Turchyn M.V. Ocular manifestations of Lyme borreliosis: current state and future perspectives. Achievements of Clinical and Experimental Medicine. 2025;3:29-37. doi: 10.11603/1811-2471.2025.v.i3.15551 (In Ukrainian).
- Tijsse-Klasen E., Pandak N., Hengeveld P. et al. Ability to cause erythema migrans differs between Borrelia burgdorferi sensu lato isolates. Parasites & Vectors. 2013;6(23). doi: 10.1186/1756-3305-6-23.
- Міщенко В.А., Рибалко Г.М., Яковенко Д.В. та ін. Системний кліщовий бореліоз у дітей. Навч.-метод. посібник для самостійної роботи лікарів. 2019. 40 с.
- Myszkowska-Torz A., Tomaszewski M., Kotowski M. et al. Cutaneous Manifestations of Lyme Borreliosis in Children — A Case Series and Review. Life (Basel). 2022 Dec 27;13(1):72. doi: 10.3390/life13010072.
- Steere A.C., Dhar A., Hernandez J. et al. Systemic symptoms without erythema migrans as the presenting picture of early Lyme disease. Am J Med. 2003 Jan;114(1):58-62. doi: 10.1016/s0002-9343(02)01440-7.
- Aucott J., Morrison C., Munoz B. et al. Diagnostic challenges of early Lyme disease: lessons from a community case series. BMC Infect Dis. 2009 Jun 1;9:79. doi: 10.1186/1471-2334-9-79.
- Andreychyn M.A., Korda M.M., Kopcha V.S. et al. Method of diagnosis of non-erythematous Lyme Disease. Infectious disease. 2020;(1):16-19. doi: 10.11603/1681-2727.2020.1.11092 (In Ukrainian).
- Nadeem M., Tafader A., Markley J.D. et al. Liver manifestations of tick-borne diseases. Clin Liver Dis (Hoboken). 2023 Mar 20;21(4):111-116. doi: 10.1097/CLD.0000000000000025.
- Lytvyn H., Basa N., Slivinska-Kurchak K. et al. First-degree atrioventricular block in 14-year-old child due to Lyme disease. J Infect Dev Ctries. 2022 Apr 30;16(4):726-728. doi: 10.3855/jidc.15071.
- Bellafiore J., Mahrous A., Gurumurthy V. et al. Retrospective Case Series of Ocular Lyme Disease, 1988-2025. Emerg Infect Dis. 2026 Jan;32(1):15-20. doi: 10.3201/eid3201.250769.