
Архив офтальмологии Украины Том 14, №1, 2026
Вернуться к номеру
Оптимізація корекції анофтальмічного синдрому
Авторы: Путієнко О.О., Петренко І.М., Денисюк Л.І.
Національний університет охорони здоров’я України імені П.Л. Шупика, м. Київ, Україна
Рубрики: Офтальмология
Разделы: Клинические исследования
Версия для печати
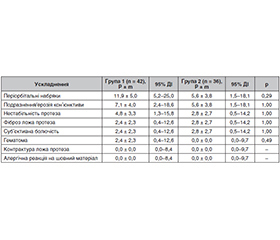
Актуальність. Анофтальмічний синдром супроводжується вираженими анатомічними, функціональними та психоемоційними порушеннями, що суттєво знижують якість життя пацієнтів. Незважаючи на розвиток реконструктивної хірургії та застосування орбітальних імплантів, досягнення стабільного морфометричного та естетичного результату залишається складним завданням, особливо у разі дефіциту м’яких тканин орбіти. Сучасні підходи потребують поєднання імплантації з методами м’якотканинної реконструкції для забезпечення оптимального функціонального та косметичного ефекту. Мета: визначити ефективність оптимізованого методу корекції анофтальмічного синдрому. Матеріали та методи. У дослідження включено 78 пацієнтів з анофтальмічним синдромом (42 — реконструкція м’яких тканин орбіти з використанням інтраорбітального імпланта; 36 — реконструкція з додатковим застосуванням ліпофілінгу), яким проводили комплексне клінічне та морфометричне обстеження, включаючи огляд, біомікроскопію та комп’ютерну томографію орбіт. Хірургічне лікування передбачало встановлення інтраорбітального імпланта, а при застосуванні ліпофілінгу — додаткове введення автологічної жирової тканини в орбітальну та періорбітальну ділянки для відновлення об’єму та поліпшення естетичного результату. Косметичну задоволеність визначали за VAS, психологічний стан — за HADS (підшкали тривоги та депресії). Динаміку показників відстежували через 3, 6, 12 місяців після операції. Статистичний аналіз виконано методами описової та аналітичної статистики з використанням t-критерію Стьюдента, точного критерію Фішера та рівня значущості p < 0,05. Результати. У пацієнтів, яким проводили реконструкцію м’яких тканин орбіти з використанням інтраорбітального імпланта, через 12 місяців після операції об’єм орбіти збільшився з 19,1 ± 3,0 см3 до 21,8 ± 2,5 см3, а товщина м’яких тканин — з 4,4 ± 0,8 мм до 5,6 ± 0,4 мм (p < 0,05); рівень косметичної задоволеності поліпшився у 2,1 раза, а рівень тривоги знизився у 2,25 раза (p < 0,05). Реконструкція м’яких тканин орбіти з використанням інтраорбітального імпланта з ліпофілінгом забезпечила більш виражений ефект: об’єм орбіти зріс з 19,0 ± 2,8 см3 до 23,7 ± 1,8 см3, товщина м’яких тканин — з 4,5 ± 0,7 мм до 6,4 ± 0,4 мм (p < 0,05), рівень косметичної задоволеності поліпшився у 2,3 раза, а рівень тривоги знизився у 3,2 раза. В обох підходах переважали легкі післяопераційні ускладнення, зокрема періорбітальні набряки, подразнення кон’юнктиви, нестабільність протеза, поодинокі випадки фіброзу ложа протеза та суб’єктивної болючості; при застосуванні методики з ліпофілінгом відзначалась тенденція до їх меншої частоти. Висновки. Обидва методи хірургічної корекції анофтальмічного синдрому є ефективними та забезпечують суттєве поліпшення морфометричних, косметичних і психоемоційних показників при високому рівні безпеки. Водночас реконструкція м’яких тканин орбіти з використанням інтраорбітального імпланта з ліпофілінгом демонструє більш виражений клінічний ефект і може розглядатися як перспективний підхід у хірургічній реконструкції анофтальмічного синдрому.
Background. Anophthalmic syndrome is accompanied by pronounced anatomical, functional, and psycho-emotional disturbances that significantly reduce the quality of life of patients. Despite advances in reconstructive surgery and the use of orbital implants, achieving a stable morphometric and aesthetic result remains a challenging task, especially in the presence of orbital soft tissue deficiency. Modern approaches require a combination of implantation with methods of soft tissue reconstruction to ensure an optimal functional and cosmetic effect. The purpose was to determine the effectiveness of an optimized method for the correction of anophthalmic syndrome. Materials and methods. The study included 78 patients with anophthalmic syndrome: 42 of them underwent reconstruction of orbital soft tissues with an intraorbital implant, 36 had reconstruction with additional use of lipofilling. A comprehensive clinical and morphometric examination, including inspection, biomicroscopy, and orbital computed tomography, were performed. Surgical treatment involved intraorbital implantation, and in cases of lipofilling — additional injection of autologous adipose tissue into the orbital and periorbital regions to restore volume and improve the aesthetic result. Cosmetic satisfaction was determined using the visual analogue scale, psychological status — with the Hospital Anxiety and Depression Scale (anxiety and depression subscales). The dynamics of indicators were monitored at 3, 6, and 12 months after surgery. Statistical analysis was performed using descriptive and analytical statistical methods, including Student’s t-test, Fisher’s exact test, with a significance level of p < 0.05. Results. In patients who underwent reconstruction of orbital soft tissues with an intraorbital implant, the orbital volume increased from 19.1 ± 3.0 to 21.8 ± 2.5 cm3 one year after surgery, and soft tissue thickness — from 4.4 ± 0.8 to 5.6 ± 0.4 mm (p < 0.05); the level of cosmetic satisfaction improved by 2.1 times, and the level of anxiety decreased by 2.25 times (p < 0.05). Reconstruction of orbital soft tissues using an intraorbital implant with lipofilling provided a more pronounced effect: orbital volume increased from 19.0 ± 2.8 to 23.7 ± 1.8 cm3, soft tissue thickness — from 4.5 ± 0.7 to 6.4 ± 0.4 mm (p < 0.05), the level of cosmetic satisfaction improved by 2.3 times, and the level of anxiety decreased by 3.2 times. In both approaches, mild postoperative complications predominated, including periorbital edema, conjunctival irritation, prosthesis instability, isolated cases of prosthesis bed fibrosis and subjective pain; when using the technique with lipofilling, a tendency toward their lower frequency was observed. Conclusions. Both methods of surgical correction for anophthalmic syndrome are effective and provide significant improvement in morphometric, cosmetic, and psycho-emotional parameters with a high level of safety. At the same time, reconstruction of orbital soft tissues using an intraorbital implant with lipofilling demonstrates a more pronounced clinical effect and can be considered a promising approach in the surgical reconstruction of anophthalmic syndrome.
анофтальмічний синдром; реконструкція орбіти; інтраорбітальні імпланти; ліпофілінг
anophthalmic syndrome; orbital reconstruction; intraorbital implants; lipofilling
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Wei DYW, Pan JT, Ming SY, Sundar G. Anophthalmic sockets: a retrospective review of enucleations, eviscerations, and exenterations performed and managed in a tertiary care hospital. J Clin Med. 2025;14(21):7764. doi: 10.3390/jcm14217764.
- Meer E, Miller AC, Ahmad M, et al. Quality of life in patients with acquired anophthalmia using an ocular prosthesis. Ophthalmic Plast Reconstr Surg. 2025;41(1):67-77. doi: 10.1097/IOP.0000000000002722.
- Hihara M, Kakudo N, Mitsui T, Kuro A, Kusumoto K. The anatomic classification of the anophthalmic eye socket (Types 0-V): a high-level taxonomy classification system. J Plast Reconstr Aesthet Surg. 2022;75(9):3491-3498. doi: 10.1016/j.bjps.2022.06.011.
- Alabdulrazaq ES, Gurnani B. Anophthalmic socket. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024.
- Fu L, Patel BC. Enucleation. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023.
- Jonak K, Matysiak M, Choragiewicz T, et al. War-related eye trauma: a study of civilian and military cases from Ukraine’s ongoing conflict. Front Public Health. 2025;13:1489445. doi: 10.3389/fpubh.2025.1489445.
- Rana V, Patra VK, Bandopadhayay S, et al. Combat ocular trauma in counterinsurgency operations. Indian J Ophthalmol. 2023;71(12):3615-3619. doi: 10.4103/IJO.IJO_609_23.
- Lee I, Davis B, Purt B, DesRosiers T. Ocular trauma and traumatic brain injury on the battlefield: a systematic review after 20 years of fighting the Global War on Terror. Mil Med. 2023;188(9-10):2916-2923. doi: 10.1093/milmed/usac226.
- Wu KY, Fujioka JK, Daigle P, Tran SD. The use of functional biomaterials in aesthetic and functional restoration in orbital surgery. J Funct Biomater. 2024;15(2):33. doi: 10.3390/jfb15020033.
- Rokohl AC, Kopecky A, Trester M, Wawer Matos PA, Pine KR, Heindl LM. Post-enucleation socket syndrome: a novel pathophysiological definition. Graefes Arch Clin Exp Ophthalmol. 2022;260(8):2427-2431. doi: 10.1007/s00417-022-05648-z.
- Lorenzano D, Chierigo A, Modugno AC. Dry anophthalmic socket syndrome: a narrative review. J Clin Med. 2025;14(24):8814. doi: 10.3390/jcm14248814.
- Al Eid S, AlSulaiman HM, Elkhamary SM, et al. Superior rectus/levator complex in acquired anophthalmic socket repaired with spheric implant: a computed tomography scan and topographic study. Int J Ophthalmol. 2024;17(8):1483-1488. doi: 10.18240/ijo.2024.08.14.
- Quaranta-Leoni FM, Fiorino MG, Quaranta-Leoni F, Di Marino M. Anophthalmic socket syndrome: prevalence, impact and management strategies. Clin Ophthalmol. 2021;15:3267-3281. doi: 10.2147/OPTH.S325652.
- Heindl LM, Trester M, Guo Y, et al. Anxiety and depression in patients wearing prosthetic eyes. Graefes Arch Clin Exp Ophthalmol. 2021;259(2):495-503. doi: 10.1007/s00417-020-04908-0.
- Han LS, Keillor RB, Weatherhead RG. Case series of shrinking hydroxyapatite orbital implants. Br J Ophthalmol. 2021;105(10):1338-1340. doi: 10.1136/bjophthalmol-2021-319397.
- Ruiters S, Mombaerts I. The prevalence of anophthalmic socket syndrome and its relation to patient quality of life. Eye (Lond). 2021;35(7):1909-1914. doi: 10.1038/s41433-020-01178-2.
- Sarubbi C, Yaïci R, Belafkih K, et al. Cohort study of glo–bal, psychological, and visual quality of life one year after evisce–ration/enucleation surgery: QOLAE 1 study. Indian J Ophthalmol. 2025;73(12):1813-1818. doi: 10.4103/IJO.IJO_544_25.
- Calluaud G, Amelot A, Kulker D, Laure B, Pare A. Management of post enucleation socket syndrome patients: a retrospective study. J Craniomaxillofac Surg. 2022;50(2):163-169. doi: 10.1016/j.jcms.2021.12.007.
- Quigley C, Elshelmani H, Fajin G, et al. Socket outcomes following enucleation for uveal melanoma: post enucleation socket syndrome can be challenging. Eye (Lond). 2024;38(1):192-197. doi: 10.1038/s41433-023-02657-y.
- Leatherbarrow B, Jones PF, editors. Oculoplastic surgery. 3rd ed. Stuttgart: Georg Thieme Verlag; 2019. Р. 486-497.
- Garrido-Hermosilla AM, Martinez-Alberquilla I, Diaz-Ruiz MC, Monge-Carmona R, Mendez-Muros M, Sanchez-Margalet V, et al. Experience using a new high-density polyethylene-based porous orbital implant: explorative 1-year performance and safety results. Prosthesis. 2024;6:1400-1409. doi: 10.3390/prosthesis6060101.
- Dhiman S, Dwibedy A, Gaonkar T, Kenia R. Comprehensive review on management of contracted anophthalmic socket: advances and clinical insights. Odisha J Ophthalmol. 2024;31(2):55-62. doi: 10.4103/odjo.odjo_10_25.
- Chen XY, Yang X, Fan XL. The evolution of orbital implants and current breakthroughs in material design, selection, characterization, and clinical use. Front Bioeng Biotechnol. 2022;9:800998. doi: 10.3389/fbioe.2021.800998.
- Yadav NK, Priya P, Sajimon S, Sadaphale SV. Evolution of contracted socket reconstruction by ocular prosthesis and implants: a systematic review. Int J Ophthalmol Eye Disord. 2025;7(2):06-13. doi: 10.33545/26649713.2025.v7.i2a.15.
- Schellini SA. Perspectives on the clinical feasibility of techniques used in anophthalmic socket reconstruction. Expert Rev Ophthalmol. 2023;18(4):227-230. doi: 10.1080/17469899.2023.2258283.
- Rokohl AC, Pine KR, Pine NS, et al. Prosthetic eye care: The current state of the art. Prog Retin Eye Res. 2025;105:101337. doi: 10.1016/j.preteyeres.2025.101337.
- Ng LH, Chan LY, Mohamad NF, Rahmat JB. Anophthalmic socket in retinoblastoma: exploring complications and risk factors in a tertiary centre in Malaysia. Eur J Ophthalmol. 2024;34(4):999-1008. doi: 10.1177/11206721231219530.
- Aryasit O, Panyavisitkul Y, Damthongsuk P, Singha P, Rattanalert N. Factors affecting anophthalmic socket reconstruction outcomes using autologous oral mucosal graft. BMC Ophthalmol. 2024;24(1):150. doi: 10.1186/s12886-024-03301-3.
- Jovanovic N, Carniciu AL, Russell WW, Jarocki A, Kahana A. Reconstruction of the orbit and anophthalmic socket using the dermis fat graft: a major review. Ophthalmic Plast Reconstr Surg. 2020;36(6):529-539. doi: 10.1097/IOP.0000000000001610.
- Sidhu N, Agrawal S, Pushker N, Bhari N, Meel R, Bajaj MS. Autologous fat transfer for orbital volume augmentation in sockets with small nonseeing eyes. J Plast Reconstr Aesthet Surg. 2023;82:170-175. doi: 10.1016/j.bjps.2023.02.024.
- Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361-370. doi: 10.1111/j.1600-0447.1983.tb09716.x.
- Huskisson EC. Measurement of pain. Lancet. 1974;2(7889):1127-1131. doi: 10.1016/S0140-6736(74)90884-8.