
Журнал "Гастроэнтерология" Том 60, №2, 2026
Вернуться к номеру
Синдром подразненого кишечника та функціональний запор: можливості лікувального харчування при розладах кишково-мозкової взаємодії
Авторы: Губська О.Ю., Ваньчицький А.О., Ткаченко В.І., Кірієнко В.Т., Кузьмінець А.А., Панін А.В., Денесюк О.Р.
Національний медичний університет імені О.О. Богомольця, м. Київ, Україна
Рубрики: Гастроэнтерология
Разделы: Клинические исследования
Версия для печати
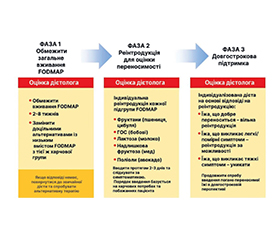
Розлади кишково-мозкової взаємодії (РКМВ), зокрема синдром подразненого кишечника (СПК) і функціональний запор, є поширеними станами, їх глобальна поширеність оцінюється як 4,1 і 11,7 % відповідно. Більшість пацієнтів визначають їжу як основний тригер симптомів цих захворювань, що робить дієтичні втручання базисом терапії РКМВ. У цій статті розглянуто сучасні дієтичні підходи при РКМВ. Загальні рекомендації щодо раціонального харчування, такі як настанови Національного інституту здоров’я (NICE) і Британської дієтологічної асоціації (BDA), використовуються як терапія першої лінії. У свою чергу дієта з низьким вмістом FODMAP (LFD) є вторинною стратегією при стійкій симптоматиці. Окремо висвітлено роль харчових волокон, серед яких доведену клінічну ефективність при СПК має лише псиліум. LFD є трьохетапним протоколом, що включає фазу обмеження, реінтродукцію та персоналізацію раціону. Метааналізи підтверджують її перевагу над іншими дієтичними втручаннями щодо зменшення загальних симптомів, абдомінального болю та здуття. Довгострокові дослідження свідчать, що 57–67 % пацієнтів досягають стійкого полегшення симптомів при дотриманні персоналізованої LFD протягом 6–12 місяців. Водночас варто підкреслити, що подібні дієтичні втручання потребують супроводу кваліфікованого дієтолога, а індивідуалізований підхід є ключовим у досягненні тривалого терапевтичного ефекту. Метою даної статті є огляд та узагальнення сучасних даних щодо можливостей лікувального харчування при поширених розладах кишково-мозкової взаємодії, зокрема синдромі подразненого кишечника та функціональному запорі.
Disorders of gut-brain interaction (DGBI), including irritable bowel syndrome and functional constipation, are common conditions with an estimated global prevalence of 4.1 and 11.7 %, respectively. Most patients identify food as the primary trigger of their symptoms, making dietary interventions the cornerstone of DGBI management. This article reviews current dietary approaches in DGBI. General healthy diet advice, such as guidelines issued by the National Institute for Health and Care Excellence and the British Dietetic Association, serves as a first-line therapy. The low-FODMAP diet (LFD), in turn, is used as a second-line strategy for patients with persistent symptoms. The role of dietary fiber is also examined, with psyllium being the only supplement to demonstrate consistent clinical efficacy in irritable bowel syndrome. LFD follows a structured three-phase protocol encompassing a restriction phase, reintroduction, and dietary personalization. Meta-analyses confirm its superiority over other dietary interventions in reducing general symptoms, abdominal pain, and bloating. Long-term studies indicate that 57–67 % of patients achieve sustained symptom relief when adhering to a personalized LFD over a period of 6–12 months. It should be emphasized that such dietary interventions require guidance from a qualified dietitian, and that an individualized approach is key to achieving lasting therapeutic outcomes. The purpose was to review and summarize current evidence on the effectiveness of medical nutrition therapy in common disorders of gut-brain interaction, particularly irritable bowel syndrome and functional constipation.
розлади кишково-мозкової взаємодії; синдром подразненого кишечника; функціональний запор; дієтичні втручання; дієта з низьким вмістом FODMAP
disorders of gut-brain interaction; irritable bowel syndrome; functional constipation; dietary interventions; low-FODMAP diet
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Mearin F, Lacy B, Chang L, et al. Rome IV: The functional bowel disorders. Gastroenterology. 2016;150:1393-1407. DOI: 10.1053/j.gastro.2016.02.031.
- Sperber AD, Bangdiwala SI, Drossman DA, et al. Worldwide prevalence and burden of functional gastrointestinal disorders, results of Rome foundation global study. Gastroenterology. 2021;160:99-114. doi: 10.1053/j.gastro.2020.04.014.
- Bohn L, Störsrud S, Törnblom H, et al. Self-reported food-related gastrointestinal symptoms in IBS are common and associated with more severe symptoms and reduced quality of life. Am J Gastroenterol. 2013;108:634-641. doi: 10.1038/ajg.2013.105.
- Van den Houte K, Bercik P, Simren M, et al. Mechanisms underlying food-triggered symptoms in disorders of gut-brain interaction. Am J Gastroenterol. 2022;116(6):937-946. doi: 10.14309/ajg.0000000000001812.
- Hookway C, Buckner S, Crosland P, et al. Irritable bowel syndrome in adults in primary care: Summary of updated NICE guidance. BMJ. 2015;350:h701. doi: 10.1136/bmj.h701.
- McKenzie YA, Bowyer RK, Leach H, et al. British Dietetic Association systematic review and evidence-based practice guidelines for the dietary management of irritable bowel syndrome in adults (2016 update). J Hum Nutr Diet. 2016;29:549-575. doi: 10.1111/jhn.12385.
- Black CJ, Staudacher HM, Ford AC. Efficacy of a low FODMAP diet in irritable bowel syndrome: Systematic review and network meta-analysis. Gut. 2021;10:2021-325214. doi: 10.1136/gutjnl-2021-325214.
- Eswaran SL, Chey WD, Han-Markey T, et al. A randomi–zed controlled trial comparing the low FODMAP diet vs. modified NICE guidelines in US adults with IBS-D. Am J Gastroenterol. 2016;111:1824-1832. doi: 10.1038/ajg.2016.434.
- Bohn L, Störsrud S, Liljebo T, et al. Diet low in FODMAPs reduces symptoms of irritable bowel syndrome as well as traditio–nal dietary advice: A randomized controlled trial. Gastroenterology. 2015;149(6):1399-1407.e2. doi: 10.1053/j.gastro.2015.07.054.
- So D, Gibson PR, Muir JG, et al. Dietary fibres and IBS: Translating functional characteristics to clinical value in the era of personalised medicine. Gut. 2021;70:2383-2394. doi: 10.1136/gutjnl-2021-324891.
- Murphy N, Norat T, Ferrari P, et al. Dietary fibre intake and risks of cancers of the colon and rectum in the European prospective investigation into cancer and nutrition (EPIC). PLoS One. 2012;7:e39361. doi: 10.1371/journal.pone.0039361.
- Ford AC, Moayyedi P, Chey WD, et al. American College of Gastroenterology monograph on management of irritable bowel syndrome. Am J Gastroenterol. 2018;113:1-18. doi: 10.1038/s41395-018-0084-x.
- Wilson B, Rossi M, Dimidi E, et al. Prebiotics in irritable bo–wel syndrome and other functional bowel disorders in adults: A systematic review and meta-analysis of randomized controlled trials. Am J Clin Nutr. 2019;109:1098-1111. doi: 10.1093/ajcn/nqy376.
- Gill SK, Rossi M, Bajka B, et al. Dietary fibre in GI health and disease. Nat Rev Gastroenterol Hepatol. 2021;18:101-116. doi: 10.1038/s41575-020-00375-4.
- Gibson PR, Halmos EP, Muir JG. Review article: FODMAPs, prebiotics and gut health — the FODMAP hypothesis revisited. Aliment Pharmacol Ther. 2020;52:233-246. doi: 10.1111/apt.15818.
- Hustoft TN, Hausken T, Ystad SO, et al. Effects of varying dietary content of fermentable short-chain carbohydrates on symptoms, fecal microenvironment, and cytokine profiles in patients with irritable bowel syndrome. Neurogastroenterol Motil. 2017;29:e12969. doi: 10.1111/nmo.12969.
- So D, Yao CK, Ardalan ZS, et al. Supplementing dietary fibers with a low FODMAP diet in irritable bowel syndrome: A randomized controlled crossover trial. Clin Gastroenterol Hepatol. 2021;18:S1542-3565. doi: 10.1016/j.cgh.2021.12.016.
- So D, Yao CK, Gibson PR, et al. Evaluating tolerability of resistant starch 2, alone and in combination with minimally fermented fibre for patients with irritable bowel syndrome: A pilot randomised controlled cross-over trial. J Nutr Sci. 2022;11:e15. doi: 10.1017/jns.2022.9.
- Gunn D, Abbas Z, Harris HC, et al. Psyllium reduces inu–lin-induced colonic gas production in IBS: MRI and in vitro fermentation studies. Gut. 2022;71:919-927. doi: 10.1136/gutjnl-2021-324784.
- Holtmann GJ, Ford AC, Talley NJ. Pathophysiology of irritable bowel syndrome. Lancet Gastroenterol Hepatol. 2016;1:133-146. doi: 10.1016/S2468-1253(16)30023-1.
- Dimidi E, Christodoulides S, Scott SM, et al. Mechanisms of action of probiotics and the gastrointestinal microbiota on gut motility and constipation. Adv Nutr. 2017;8(3):484-94. doi: 10.3945/an.116.014407.
- Ford AC, Harris LA, Lacy BE, et al. Systematic review with meta-analysis: The efficacy of prebiotics, probiotics, synbiotics and antibiotics in irritable bowel syndrome. Aliment Pharmacol Ther. 2018;48(10):1044-60. doi: 10.1111/apt.15001.
- Hod K, Ringel Y, van Tilburg MAL, et al. Pathophysiology of IBS: Rationale for the use of probiotics as a treatment for IBS. J Clin Med. 2021;10(17):3793.
- McFarland LV, Dublin S. Meta-analysis of probiotics for the treatment of irritable bowel syndrome. World J Gastroenterol. 2008;14(17):2650-61. doi: 10.3748/wjg.14.2650.
- Hungin APS, Mulligan C, Pot B, et al. Systematic review: Probiotics in the management of lower gastrointestinal symptoms in clinical practice — an evidence-based international guide. Aliment Pharmacol Ther. 2013;38(8):864-86. doi: 10.1111/apt.12460.
- Didari T, Mozaffari S, Nikfar S, et al. Effectiveness of probiotics in irritable bowel syndrome: Updated systematic review with meta-analysis. World J Gastroenterol. 2015;21(10):3072-84. doi: 10.3748/wjg.v21.i10.3072.
- Wilkins T, Sequoia J. Probiotics for gastrointestinal conditions: A summary of the evidence. Am Fam Physician. 2017;96(3):170-8.
- Zhang Y, Li L, Guo C, et al. Effects of probiotic type, dose and treatment duration on irritable bowel syndrome diagnosed by Rome III criteria: A meta-analysis. BMC Gastroenterol. 2016;16(1):62. doi: 10.1186/s12876-016-0470-z.
- Ford AC, Quigley EMM, Lacy BE, et al. Efficacy of prebio–tics, probiotics, and synbiotics in irritable bowel syndrome and chronic idiopathic constipation: Systematic review and meta-analysis. Am J Gastroenterol. 2014;109(10):1547-61. doi: 10.1038/ajg.2014.202.
- Lyra A, Hillilä M, Huttunen T, et al. Irritable bowel syndrome symptom severity improves equally with probiotic and placebo. World J Gastroenterol. 2016;22(48):10631-42. doi: 10.3748/wjg.v22.i48.10631.
- Gwee KA, Lee WS, Ling KL, et al. Consensus guidelines on the use of probiotics in clinical practice: Expert panel of the Asia-Pacific Association of Gastroenterology. J Gastroenterol Hepatol. 2018;33(3):752-62. doi: 10.1111/jgh.14268.
- Enck P, Mazurak N. Dysbiosis in functional bowel disorders. Ann Nutr Metab. 2018;72(4):296-306. doi: 10.1159/000488773.
- Pinto-Sanchez MI, Hall GB, Ghajar K, et al. Probiotic Bifidobacterium longum NCC3001 reduces depression scores and alters brain activity: A pilot study in patients with irritable bowel syndrome. Gastroenterology. 2017;153(2):448-59.e8. doi: 10.1053/j.gastro.2017.05.003.
- Stepanova M, Rodriguez E, Birerdinc A, et al. Nonalcoholic fatty liver disease and cognitive function: A systematic review. J Hepatol. 2018;68(6):1258-64. doi: 10.21037/tgh.2019.08.09.
- Dimidi E, Zdanaviciene A, Christodoulides S, et al. Randomised clinical trial: Bifidobacterium lactis BB-12 and Lactobacillus plantarum LP01 in the management of irritable bowel syndrome. Benef Microbes. 2019;10(3):267-76.
- Martoni CJ, Srivastava S, Leyer GJ. Lactobacillus acidophi–lus DDS-1 and Bifidobacterium lactis UABla-12 improve abdominal pain severity and symptomology in IBS: Randomized controlled trial. Benef Microbes. 2020;11(3):235-47. doi: 10.3390/nu12020363.
- Francis CY, Morris J, Whorwell PJ. The irritable bowel severity scoring system: A simple method of monitoring irritable bowel syndrome and its progress. Aliment Pharmacol Ther. 1997;11(2):395-402. doi: 10.1046/j.1365-2036.1997.142318000.x.
- Lewis SJ, Heaton KW. Stool form scale as a useful guide to intestinal transit time. Scand J Gastroenterol. 1997;32(9):920-4. doi: 10.3109/00365529709011203.
- Francis CY, Whorwell PJ. Bran and irritable bowel syndrome: Time for reappraisal. Lancet. 1994;344(8914):39-40. doi: 10.1016/s0140-6736(94)91055-3.
- Rao SSC, Yu S, Fedewa A. Systematic review: Dietary fibre and FODMAP-restricted diet in the management of constipation and irritable bowel syndrome. Aliment Pharmacol Ther. 2015;41(12):1256-70. doi: 10.1111/apt.13167.
- Tuck CJ, Vanner S. Dietary therapies in IBS. Gastroenterol Clin North Am. 2021;50(3):519-36. doi: 10.1111/nmo.13238.
- Bijkerk CJ, Muris JWM, Knottnerus JA, et al. Systematic review: The role of different types of fibre in the treatment of irritable bowel syndrome. Aliment Pharmacol Ther. 2004;19(3):245-51. doi: 10.1111/j.0269-2813.2004.01862.x.
- Staudacher HM, Irving PM, Lomer MCE, et al. Mechanisms and efficacy of dietary FODMAP restriction in IBS. Nat Rev Gastroenterol Hepatol. 2014;11(4):256-66. doi: 10.1038/nrgastro.2013.259.
- Skodje GI, Sarna VK, Minelle IH, et al. Fructan, rather than gluten, induces symptoms in patients with self-reported non-celiac gluten sensitivity. Gastroenterology. 2018;154(3):529-39.e2. doi: 10.1053/j.gastro.2017.10.040.
- Staudacher HM, Whelan K, Irving PM, et al. Comparison of symptom response following advice for a diet low in fermentable carbohydrates (FODMAPs) versus standard dietary advice in patients with IBS. J Hum Nutr Diet. 2011;24(5):487-95. doi: 10.1111/j.1365-277X.2011.01162.x.
- Hustoft TN, Hausken T, Ystad SO, et al. A diet low in FODMAPs reduces symptoms of IBS. World J Gastroenterol. 2017;23(18):3356-66. doi: 10.1053/j.gastro.2013.09.046.
- De Roest RH, Dobbs BR, Chapman BA, et al. The low FODMAP diet improves gastrointestinal symptoms in patients with IBS: A prospective study. Int J Clin Pract. 2013;67(9):895-903. https://doi.org/10.1111/ijcp.12128.
- Eswaran SL, Chey WD, Jackson K, et al. A diet low in fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAPs) improves quality of life and reduces activity impairment in IBS patients. Am J Gastroenterol. 2017;112(11):1829-36. doi: 10.1016/j.cgh.2017.06.044.
- Halmos EP, Power VA, Shepherd SJ, et al. A diet low in FODMAPs reduces symptoms of IBS. Gastroenterology. 2014;146(1):67-75.e5. doi: 10.1053/j.gastro.2013.09.046.