
Журнал "Гастроэнтерология" Том 60, №2, 2026
Вернуться к номеру
Метаболічний профіль у військовослужбовців із запальними захворюваннями кишечника
Авторы: Стойкевич М.В., Кленіна І.А., Тарасова Т.С., Петішко О.П.
ДУ «Інститут гастроентерології НАМН України», м. Дніпро, Україна
Рубрики: Гастроэнтерология
Разделы: Клинические исследования
Версия для печати
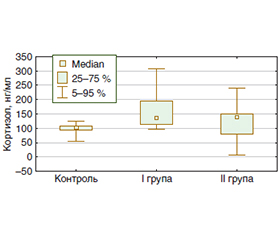
Мета дослідження: провести оцінку показників ліпідного та вуглеводного обміну, кортизолу, лептину і визначити їхні взаємозв’язки у військовослужбовців із запальними захворюваннями кишечника (ЗЗК) і метаболічним синдромом. Матеріали та методи. Обстежено 40 військовослужбовців із ЗЗК, яких розподілили на 2 групи: I група — 32 пацієнти без метаболічного синдрому, II група — 8 пацієнтів з метаболічним синдромом. Контрольну групу становили 10 практично здорових осіб. У сироватці крові визначали показники ліпідного профілю, глюкозу, інсулін, кортизол, лептин; інсулінорезистентність оцінювали за індексом HOMA-IR. Результати. У всіх хворих із ЗЗК встановлено підвищення рівня кортизолу порівняно з контролем (р < 0,05) без вірогідної різниці між групами. Рівень лептину в II групі був вищим у 2,4 раза порівняно з контролем — 6,25 (4,0; 16,2) проти 2,65 (0,45; 3,9) нг/мл, і в 1,5 раза порівняно з I групою — 4,1 (2,3; 8,4) нг/мл (р < 0,05). У I і II групах виявлено тенденцію до підвищення глюкози натще до 5,0 (4,8; 5,4) і 5,4 (4,7; 6,2) ммоль/л проти 4,4 (4,1; 4,6) ммоль/л у контролі. У пацієнтів з метаболічним синдромом рівень інсуліну становив 12,9 (7,7; 25,8) мкОД/мл, що було в 1,8 раза вище, ніж у I групі, а HOMA-IR — 3,1 (1,6; 6,0), що перевищувало показник контролю в 1,4 раза і I групи — у 2,1 раза (р < 0,05). Ліпідний профіль II групи характеризувався підвищенням холестерину до 5,22 (4,93; 5,86) ммоль/л, тригліцеридів — до 1,44 (1,29; 2,11) ммоль/л, ліпопротеїнів дуже низької щільності — до 0,66 (0,59; 0,97) ммоль/л і зниженням ліпопротеїнів високої щільності до 1,17 (0,87; 1,41) ммоль/л. Встановлено прямий зв’язок HOMA-IR з кортизолом (r = +0,369; p = 0,033) і лептину — з HOMA-IR (r = +0,437; p = 0,005). Висновки. У військовослужбовців із ЗЗК наявність метаболічного синдрому асоціюється з більш вираженими порушеннями вуглеводного та ліпідного обміну, підвищенням лептину і формуванням інсулінорезистентності. Включення до стандартного обстеження показників інсуліну, HOMA-IR, лептину та кортизолу може покращити ранню діагностику метаболічної коморбідності та стратифікацію ризику.
Background. The purpose of the study was to assess the indicators of lipid and carbohydrate metabolism, cortisol, leptin, and their relationships in military personnel with inflammatory bowel disease and metabolic syndrome. Materials and methods. The study included 40 military personnel with inflammatory bowel disease, who were divided into 2 groups: group I comprised 32 participants without metabolic syndrome, and group II included 8 patients with metabolic syndrome. The control group consisted of 10 apparently healthy individuals. Serum lipid parameters, glucose, insulin, cortisol, and leptin levels were measured. Insulin resistance was assessed using the HOMA-IR index. Results. All patients with inflammatory bowel disease demonstrated elevated serum cortisol compared to the control group (p < 0.05), with no significant difference between the study groups. Leptin levels in group II were 2.4-fold higher than in the control group, amounting to 6.25 (4.0; 16.2) ng/mL versus 2.65 (0.45; 3.9) ng/mL, and 1.5-fold higher than in group I, in which the content was 4.1 (2.3; 8.4) ng/mL (p < 0.05). Fasting glucose tended to increase in both groups I and II, reaching 5.0 (4.8; 5.4) mmol/L and 5.4 (4.7; 6.2) mmol/L, respectively, versus 4.4 (4.1; 4.6) mmol/L in controls. In patients with metabolic syndrome, insulin level was 12.9 (7.7; 25.8) μIU/mL, which was 1.8-fold higher than in group I, while HOMA-IR was 3.1 (1.6; 6.0), exceeding the control value by 1.4-fold and the group I value by 2.1-fold (p < 0.05). The lipid profile in group II was characterized by total cholesterol increase to 5.22 (4.93; 5.86) mmol/L, triglycerides to 1.44 (1.29; 2.11) mmol/L, and very low-density lipoprotein cholesterol to 0.66 (0.59; 0.97) mmol/L, along with a decrease in high-density lipoprotein cholesterol to 1.17 (0.87; 1.41) mmol/L. A direct correlation was found between HOMA-IR and cortisol levels (r = +0.369; p = 0.033), as well as between leptin and HOMA-IR (r = +0.437; p = 0.005). Conclusions. In military personnel with inflammatory bowel disease, the presence of metabolic syndrome is associated with more pronounced disturbances in carbohydrate and lipid metabolism, elevated leptin levels, and the development of insulin resistance. Incorporating insulin, HOMA-IR, leptin, and cortisol assessment into the standard examination may improve early diagnosis of metabolic comorbidity and risk stratification.
запальні захворювання кишечника; військовослужбовці; метаболічний синдром; ліпідний обмін; вуглеводний обмін; інсулінорезистентність; HOMA-IR; кортизол; лептин
inflammatory bowel disease; military personnel; metabolic syndrome; lipid metabolism; carbohydrate metabolism; insulin resistance; HOMA-IR; cortisol; leptin
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Sun Y, Zhang Z, Zheng CQ, Sang LX. Mucosal lesions of the upper gastrointestinal tract in patients with ulcerative colitis: A review. World Journal of Gastroenterology. 2021;27(22):2963-2978. DOI: https://doi.org/10.3748/wjg.v27.i22.2963.
- Hatch-McChesney A, Smith TJ. Nutrition, Immune Function, and Infectious Disease in Military Personnel: A Narrative Review. Nutrients. 2023;15(23):4999. DOI: https://doi.org/10.3390/nu15234999.
- Collier KM, McGuire C. Nutritional vulnerabilities in military personnel under chronic operational stress. Military Medicine. 2024;189(1-2):e112-e119. DOI: https://doi.org/10.1093/milmed/usaa999.
- Dunleavy KA, Raffals LE, Camilleri M. Intestinal Barrier Dysfunction in Inflammatory Bowel Disease: Underpinning Pathogenesis and Therapeutics. Dig Dis Sci. 2023;68(12):4306-4320. DOI: https://doi.org/10.1007/s10620-023-08122-w.
- Lopes MA, Oliveira ECS, Quaglio AEV, et al. From gut to liver: Exploring the relationship between inflammatory bowel disease and metabolic dysfunction-associated steatotic liver disease. World J Hepatol. 2025;17(9):109035. DOI: https://doi.org/10.4254/wjh.v17.i9.109035.
- Davenport M, Poles J, Leung JM, et al. Metabolic alterations to the mucosal microbiota in inflammatory bowel disease. Inflamm Bowel Dis. 2014;20(4):723-31. DOI: https://doi.org/10.1097/MIB.0000000000000011.
- Chen H, Li W, Hu J, et al. Association of serum lipids with inflammatory bowel disease: a systematic review and meta-analysis. Front Med (Lausanne). 2023;10:1198988. doi: https://doi.org/10.3389/fmed.2023.1198988.
- Kang S, Jeong DY, Seo J, Daily JW, Park S. Microbiota-Mediated Bile Acid Metabolism as a Mechanistic Framework for Precision Nutrition in Gastrointestinal and Metabolic Diseases. Cells. 2025;15(1):23. DOI: https://doi.org/10.3390/cells15010023.
- Hyun HK, Cheon JH. Metabolic Disorders and Inflammatory Bowel Diseases. Gut Liver. 2025;19(3):307-317. doi: https://doi.org/10.5009/gnl240316.
- Habib MB, Akbar NS, Batool G. Investigation of Dyslipide–mia and Lipid Profile Ratios Among Patients in Tertiary Care Hospitals. EJIFCC. 2025;36(2):124-131. PMID: 40590036; PMCID: PMC12208299.
- Chen Y, Chen X, Lin S, et al. Effects of psychological stress on inflammatory bowel disease via affecting the microbiota-gut-brain axis. Chin Med J (Engl). 2025;138(6):664-677. DOI: https://doi.org/10.1097/CM9.0000000000003389.
- Crabb KE, Clay M, Pham U, Chinn LK, Grigorenko EL. Cortisol, stress, and cognition in military subpopulations: A systematic review and meta-analysis. Psychoneuroendocrinology. 2026;183:107679. DOI: https://doi.org/10.1016/j.psyneuen.2025.107679.
- Buccellato KH, Peterson AL. The role of cortisol in deve–lopment and treatment of PTSD among service members: A narrative review. Psychoneuroendocrinology. 2024;169:107152. DOI: https://doi.org/10.1016/j.psyneuen.2024.107152.
- Obradovic M, Sudar-Milovanovic E, Soskic S, et al. Leptin and Obesity: Role and Clinical Implication. Front Endocrinol (Lausanne). 2021;12:585887. DOI: https://doi.org/10.3389/fendo.2021.585887.
- Pereira S, Cline DL, Glavas MM, Covey SD, Kieffer TJ. Tissue-Specific Effects of Leptin on Glucose and Lipid Metabolism. Endocr Rev. 2021;42(1):1-28. DOI: https://doi.org/10.1210/endrev/bnaa027.
- Brewin CR, Atwoli L, Bisson JI, Galea S, Koenen K, Le–wis-Fernández R. Post-traumatic stress disorder: evolving conceptualization and evidence, and future research directions. World Psychiatry. 2025;24(1):52-80. DOI: https://doi.org/10.1002/wps.21269.
- Alotiby A. Immunology of Stress: A Review Article. J Clin Med. 2024;13(21):6394. DOI: https://doi.org/10.3390/jcm13216394.
- Kimhi S, Eshel Y, Marciano H, Adini B. Impact of the war in Ukraine on resilience, protective, and vulnerability factors. Front Public Health. 2023;11:1053940. DOI: https://doi.org/10.3389/fpubh.2023.1053940.
- Kurapov A, Kalaitzaki A, Keller V, Danyliuk I, Kowatsch T. The mental health impact of the ongoing Russian-Ukrainian war 6 months after the Russian invasion of Ukraine. Front Psychiatry. 2023;14:1134780. DOI: https://doi.org/10.3389/fpsyt.2023.1134780.
- Kivimäki M, Bartolomucci A, Kawachi I. The multiple roles of life stress in metabolic disorders. Nat Rev Endocrinol. 2023;19(1):10-27. DOI: https://doi.org/10.1038/s41574-022-00746-8.
- Muhie S, Gautam A, Yang R, et al. Molecular signatures of post-traumatic stress disorder in war-zone-exposed veteran and active-duty soldiers. Cell Rep Med. 2023;4(5):101045. DOI: https://doi.org/10.1016/j.xcrm.2023.101045.
- Alberti KG, Zimmet P, Shaw J. Metabolic syndrome — a new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabet Med. 2006;23(5):469-80. doi: https://doi.org/10.1111/j.1464-5491.2006.01858.x.
- Kyle UG, Earthman CP, Pichard C, Coss-Bu JA. Body composition during growth in children: limitations and perspectives of bioelectrical impedance analysis. Eur J Clin Nutr. 2015 Dec;69(12):1298-305. doi: https://doi.org/10.1038/ejcn.2015.86.