
Международный эндокринологический журнал Том 22, №4, 2026
Вернуться к номеру
Роль приєднання гормонального компонента до патогенетичної терапії мієлодиспластичного синдрому
Авторы: H.S. Starodub (1), N.V. Horiainova (1), S.V. Konovalenko (2)
(1) - National Research Center for Radiation Medicine, Hematology and Oncology of NAMSU, Kyiv, Ukraine
(2) - R.E. Kavetsky Institute of Experimental Pathology, Oncology and Radiobiology of NASU, Kyiv, Ukraine
Рубрики: Эндокринология
Разделы: Клинические исследования
Версия для печати
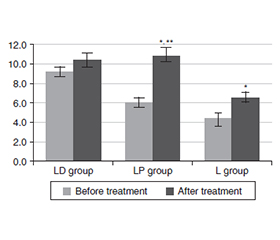
Актуальність. При мієлодиспластичному синдромі (МДС) дисбаланс інтерлейкінів викликає посилення апоптозу гемопоетичних стовбурових клітин, тобто цитопенію. Активація інфламасом внаслідок специфічних мутацій, наприклад SF3B1 або del(5q), пов’язана з різними профілями цитокінів та запальними фенотипами. Мета: оцінити рівні прозапальних і протизапальних інтерлейкінів на тлі ад’ювантної гормональної терапії в осіб із МДС. Матеріали та методи. Сформовано 3 групи клінічного спостереження, у яких хворим було призначено відповідне лікування: леналідомід за схемою монотерапії (група L), леналідомід і дексаметазон п/о табл. 3 мг на добу в перший місяць та по 1 мг у наступні 2 місяці (група LD), а також леналідомід і преднізолон п/о табл. 15 мг на добу в перший місяць та по 10 мг у наступні 2 місяці (група LP). До та після лікування (через 3 місяці) оцінювали рівні прозапальних і протизапальних цитокінів. Результати. Встановлено ефективність ад’ювантної гормональної протизапальної терапії у пацієнтів із МДС, які отримують лікування леналідомідом. Зниження рівнів прозапального IL-6 з 9,2 ± 1,1 пг/мл до 6,7 ± 0,8 пг/мл у хворих, які отримували дексаметазон, а також з 8,8 ± 1,3 пг/мл до 4,9 ± 1,8 пг/мл у тих, хто приймав преднізолон, свідчить на користь застосування гормональних препаратів з метою зменшення системного запалення при МДС. Не менш значущим для клінічної практики виявилося зниження, що продемонстрував IL-1β у групі, яка разом із леналідомідом приймала преднізолон: з 12,8 ± 2,0 пг/мл до 5,8 ± 1,3 пг/мл, результат вірогідний порівняно з показниками до лікування, а також із групою L, p < 0,05. Одночасно важливим виявилося зростання рівня протизапальних інтерлейкінів: IL-4 на тлі прийому преднізолону та IL-10 у групі хворих, яким був призначений дексаметазон. Висновки. Призначення гормональної ад’ювантної терапії обумовило зниження рівнів прозапальних інтерлейкінів і зростання — протизапальних. При цьому у групі хворих, які приймали тільки леналідомід без гормонів, концентрація TNF-α у сироватці зросла з 8,4 ± 2,0 пг/мл до 12,2 ± 2,2 пг/мл. Дослідження ефективності ад’ювантних протоколів у комплексному лікуванні МДС необхідно продовжувати, адже будь-яке терапевтичне втручання, що знижує інтенсивність системного запалення і потенційно може поліпшити якість життя хворих та прогноз захворювання, обґрунтовано заслуговує на увагу науковців і клініцистів.
Background. In myelodysplastic syndrome (MDS), an imbalance of interleukins causes increased apoptosis of hematopoietic stem cells, i.e. cytopenia. Activation of inflammasomes due to specific mutations, for example, SF3B1 or del(5q), is associated with different cytokine profiles and inflammatory phenotypes. Objective: to study the levels of pro-inflammatory and anti-inflammatory interleukins against the background of adjuvant hormonal therapy in patients with MDS. Materials and methods. Three clinical observation groups were formed, in which patients were assigned the appropriate treatment: lenalidomide according to the monotherapy regimen (L group), lenalidomide and dexamethasone p/o tablet 3 mg per day in the first month and 1 mg in the next 2 months (LD group), as well as lenalidomide and prednisolone p/o tablet 15 mg per day in the first month and 10 mg in the next 2 months (LP group). Before and after treatment (in 3 months), the levels of pro-inflammatory and anti-inflammatory cytokines were assessed. Results. The effectiveness of adjuvant hormonal anti-inflammatory therapy in patients with MDS receiving treatment with lenalidomide was established. A decrease in proinflammatory IL-6 levels from 9.2 ± 1.1 to 6.7 ± 0.8 pg/ml in participants receiving dexamethasone, and from 8.8 ± 1.3 to 4.9 ± 1.8 pg/ml in those receiving prednisone indicates the benefit of using hormonal drugs to reduce systemic inflammation in MDS. No less significant for clinical practice was a decrease demonstrated by IL-1β in the group receiving prednisone together with lenalidomide: from 12.8 ± 2.0 to 5.8 ± 1.3 pg/ml, the result is significant compared to the indicators before treatment, as well as to the L group, p < 0.05. At the same time, an important result was an increase in the level of anti-inflammatory interleukins: IL-4 against the background of taking prednisolone and IL-10 in the group of patients who were prescribed dexamethasone. Conclusions. The prescription of hormonal adjuvant therapy led to a decrease in the levels of pro-inflammatory interleukins and an increase in anti-inflammatory ones. At the same time, in the group of patients who took only lenalidomide without hormones, the concentration of TNF-α in serum increased from 8.4 ± 2.0 to 12.2 ± 2.2 pg/ml. Research on the effectiveness of adjuvant protocols in the comprehensive treatment of MDS must be continued, because any therapeutic intervention that reduces the intensity of systemic inflammation and can potentially improve the quality of life of patients and the prognosis of the disease justifiably deserves the attention of scientists and clinicians.
мієлодиспластичний синдром; IL-6; IL-1β; IL-4; IL-10; TNF-α; леналідомід; дексаметазон; преднізолон; ад’ювантна гормональна терапія
myelodysplastic syndrome; IL-6; IL-1β; IL-4; IL-10; TNF-α; lenalidomide; dexamethasone; prednisolone; adjuvant hormonal therapy
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Vallelonga V, Gandolfi F, Zampini M, Riva E, Maggioni G, Ventura D, et al. PU.1-Activated Genomic Regions Define Low-risk MDS Subsets Characterized by Immune Dysregulation and Disease Progression. Blood. 2026 Jan 15:blood.2025030760. doi: 10.1182/blood.2025030760.
- Willis C, Hejazi A, Williams VL, Comperatore C, Tantravahi S, Ali NA, et al. Treatment Patterns and Outcomes of Patients With Myelo–dysplastic Syndrome (MDS) by IPSS-R Scores at Acade–mic Cancer Centers. Adv Hematol. 2025 Nov 19;2025:9924808. doi: 10.1155/ah/9924808.
- Creignou M, Sarchi M, Bernard E, Malcovati L. Evolutionary trajectories of myelodysplastic syndromes/neoplasms. Semin Cancer Biol. 2026 Feb 4;120:16-30. doi: 10.1016/j.semcancer.2026.01.006.
- Maślińska-Gromadka K, Palusińska M, Łuczak JW, Skopek R, Kraj L, Schenk T, et al. Cell Lines in Myelodysplastic Syndromes/Neoplasms (MDS) Research: A Review of Existing Models and Their Applications. Int J Mol Sci. 2026;27(2):898. doi: 10.3390/ijms27020898.
- Kawano Y, Kawano H, LaMere MW, LaMere EA, Byun DK, McGrath KE, et al. IL-1R1 and IL-18 signals regulate mesenchymal stromal cells in an aged murine model of myelodysplastic syndromes. Blood. 2025 Apr 10;145(15):1632-1644. doi: 10.1182/blood.2024024818.
- Bănescu C, Tripon F, Muntean C. The Genetic Landscape of Myelodysplastic Neoplasm Progression to Acute Myeloid Leukemia. Int J Mol Sci. 2023;24(6):5734. doi: 10.3390/ijms24065734.
- Aoki H, Suzuki Y, Okada A, Kaneko H, Ko T, Takeda N, et al. Potential Clinical Value of Identifying Myelodysplastic Syndrome as a Cardiovascular Risk Condition. Can J Cardiol. 2026 Feb 17:S0828-282X(26)00137-6. doi: 10.1016/j.cjca.2026.02.021.
- Alhajahjeh A, Woite NL, Rolles B, Stempel JM, Mina A, Mendez L, et al. Luspatercept for patients with lower-risk myelodysplastic syndromes/neoplasms: a systematic review and meta-analysis. Blood Adv. 2025 Dec 23;9(24):6511-6523. doi: 10.1182/bloodadvances.2025017611.
- Boertjes EL, et al. MDS/AML and AML with myelodysplasia-related gene mutations: clinical and molecular similarities. Blood Adv. 2026 Feb 24;10(4):939-950. doi: 10.1182/bloodadvances.2025018408.
- Zhang Y, Yan L, Fan C, Zhao B, Chen M, Hao X, et al. Myelodysplastic syndrome progress to acute myeloid leukemia: new insights and updates. Front Immunol. 2026 Feb 4;17:1769944. doi: 10.3389/fimmu.2026.1769944.
- Niu ZY, Zhu MF, Tao M, Zhang C, Gu F, Li J. Myelodysplastic Syndrome With Complex Chromosomal Karyotype Abnormalities Complicated by Multiple Intestinal Perforations: A Case Report and Literature Review. Case Rep Gastrointest Med. 2026 Jan 8;2026:2593347. doi: 10.1155/crgm/2593347.
- Imataki O, Uemura M, Kitanaka A. Characteristics of Mye–lodysplastic Syndrome with Coagulation Abnormalities and Tailored Diagnosis and Treatment. J Pers Med. 2025 Sep 5;15(9):429. doi: 10.3390/jpm15090429.
- Pierro F, Fazio M, Murdaca G, Stagno F, Gangemi S, Allegra A. Oxidative Stress and Mitochondrial Dysfunction in Myelodysplastic Syndrome: Roles in Development, Diagnosis, Prognosis, and Treatment. Int J Mol Sci. 2025;26(13):6415. doi: 10.3390/ijms26136415.
- Thalambedu N, Mohan Lal B, Harbaugh B, Alapat DV, Gaddam M, Gentille Sanchez CG, et al. Unveiling Myelodysplastic Syndromes: Exploring Pathogenic Mechanisms and Therapeutic Advances. Cancers (Basel). 2025;17(3):508. doi: 10.3390/cancers17030508.
- Lapadat M-E, Stanca O, Berbec NM, Negotei C, Colita A. Navigating the New Era in Myelodysplastic Neoplasms: A Review of Prognostic Implications of the IPSS-M Score and 2022 WHO Classification. Hematol Rep. 2025;17(6):58. doi: 10.3390/hematolrep17060058.
- Yu S, Kim J, Kim MS. A Genetically-Informed Network Mo–del of Myelodysplastic Syndrome: From Splicing Aberrations to The–rapeutic Vulnerabilities. Genes (Basel). 2025;16(8):928. doi: 10.3390/genes16080928.
- Majcherek M, Przeorski K, Mroczkowska-Bękarciak A, Nogaj N, Szymczak D, Kopszak A, et al. Integrating Molecular Alterations with Immunophenotype and Clinical Characteristics in Myelodysplastic Syndromes: A Single-Center Study. Int J Mol Sci. 2025;26(15):7382. doi: 10.3390/ijms26157382.
- Stagno F, Mirabile G, Rizzotti P, Bottaro A, Pagana A, Gangemi S, Allegra A. Using Artificial Intelligence to Enhance Myelo–dysplastic Syndrome Diagnosis, Prognosis, and Treatment. Biomedicines. 2025;13(4):835. doi: 10.3390/biomedicines13040835.