
Международный эндокринологический журнал Том 22, №4, 2026
Вернуться к номеру
Роль андрогенів у формуванні клінічного профілю системного червоного вовчака серед чоловіків
Авторы: Ждан В.М., Ткаченко М.В., Бабаніна М.Ю., Волченко Г.В., Кир’ян О.А., Кітура Є.М., Іваницький І.В., Лебідь В.Г.
Полтавський державний медичний університет, м. Полтава, Україна
Рубрики: Эндокринология
Разделы: Клинические исследования
Версия для печати
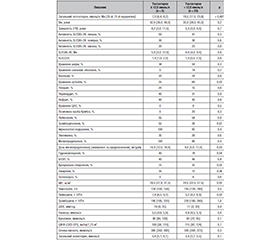
Актуальність. Системний червоний вовчак (СЧВ) у чоловіків зустрічається значно рідше, ніж у жінок, однак може характеризуватися певними клінічними особливостями. Роль андрогенів, зокрема тестостерону, у перебігу СЧВ залишається недостатньо вивченою. Дані щодо частоти гіпогонадизму та його клінічного значення при СЧВ у чоловіків є суперечливими. Мета дослідження: визначити частоту зниженого рівня тестостерону серед чоловіків із СЧВ, а також охарактеризувати особливості клінічного перебігу захворювання, специфіку застосування імуносупресивної терапії та супутні метаболічні порушення. Матеріали та методи. Проведено одномоментне клініко-лабораторне дослідження 34 чоловіків із СЧВ, які перебували на стаціонарному лікуванні протягом 2024–2025 рр. Діагноз встановлювали за критеріями SLICC (2012). Визначення загального тестостерону здійснювали методом електрохемілюмінесцентного аналізу; гіпогонадизм діагностували при рівні ≤ 12,0 нмоль/л. Оцінювали клінічні прояви, активність (SLEDAI-2K), індекс пошкодження (SLICC/DI), лабораторні показники, терапію та супутні захворювання. Для міжгрупового порівняння застосовували U-критерій Манна — Уїтні, χ2 Пірсона та кореляційний аналіз Спірмена (p < 0,05). Результати. Частота гіпогонадизму становила 14,7 %. Виявлено вірогідний зворотний зв’язок між рівнем тестостерону та дозою метилпреднізолону (в перерахунку на преднізолон) (r = –0,54; p < 0,001), а також швидкістю осідання еритроцитів (r = –0,37; p = 0,019). Позитивні кореляції встановлено між рівнем тестостерону та концентрацією гемоглобіну (r = 0,38; p = 0,015) і гематокритом (r = 0,46; p = 0,003). Пацієнти з гіпогонадизмом рідше мали ураження суглобів (25 проти 69 %; p = 0,02), отримували вищі дози глюкокортикоїдів (14,0 проти 9,0 мг/добу; p < 0,05), рідше застосовували гідроксихлорохін (40 проти 78 %; p < 0,05), характеризувалися вищим індексом маси тіла (28,5 проти 24,5 кг/м2; p < 0,05) та частішою артеріальною гіпертензією (75 проти 32 %; p < 0,05). Також у них відзначено більш виражену протеїнурію (4,5 проти 0,07 г/добу; p = 0,028) без вірогідних відмінностей у швидкості клубочкової фільтрації. Висновки. У чоловіків із СЧВ зниження рівня тестостерону асоціюється з вищими дозами глюкокортикоїдів, кардіометаболічними порушеннями та більш вираженою протеїнурією, але не пов’язане з загальною активністю захворювання. Отримані дані підкреслюють доцільність оцінки гормонального профілю у чоловіків із СЧВ та потребують підтвердження в дослідженнях із більшою вибіркою.
Background. Systemic lupus erythematosus (SLE) occurs considerably less frequently in men than in women; however, male SLE may be characterized by distinct clinical features. The role of androgens, particularly testosterone, in the course of SLE remains insufficiently elucidated. Data regarding the prevalence of hypogonadism and its clinical relevance in men with SLE are limited and inconsistent. The aim of this study was to determine the frequency of low testosterone levels among men with SLE, as well as to characterize the features of the clinical course of the disease, the specifics of using immunosuppressive therapy, and concomitant metabolic disorders. Materials and methods. A cross-sectional clinical and laboratory study included 34 men with SLE who were hospitalized in 2024–2025. The diagnosis was established according to the 2012 SLICC classification criteria. Total testosterone levels were measured using electrochemiluminescence immunoassay; hypogonadism was defined in serum testosterone ≤ 12.0 nmol/L. Clinical manifestations, disease activity (SLEDAI-2K), damage index (SLICC/DI), laboratory parameters, ongoing therapy, and comorbidities were assessed. Intergroup comparisons were performed using the Mann-Whitney U test and Pearson’s χ2 test; correlations were analyzed using Spearman’s rank coefficient (p < 0.05). Results. The prevalence of hypogonadism was 14.7 %. A significant inverse correlation was observed between testosterone levels and methylprednisolone dose (expressed as prednisone equivalent) (r = –0.54; p < 0.001), as well as erythrocyte sedimentation rate (r = –0.37; p = 0.019). Positive correlations were found between testosterone and hemoglobin concentration (r = 0.38; p = 0.015) and hematocrit (r = 0.46; p = 0.003). Patients with hypogonadism less frequently exhibited joint involvement (25 vs 69 %; p = 0.02), received higher glucocorticoid doses (14.0 vs 9.0 mg/day; p < 0.05), and were less likely to receive hydroxychloroquine (40 vs 78 %; p < 0.05). They also demonstrated higher body mass index (28.5 vs 24.5 kg/m2; p < 0.05) and a higher prevalence of hypertension (75 vs 32 %; p < 0.05). Additionally, greater proteinuria was observed in the hypogonadal group (4.5 vs 0.07 g/day; p = 0.028), without significant differences in estimated glomerular filtration rate. Conclusions. In men with SLE, reduced testosterone levels are associated with higher glucocorticoid exposure, cardiometabolic disturbances, and more pronounced proteinuria, but not with overall disease activity. These findings support the clinical relevance of hormonal evaluation in male patients with SLE and warrant confirmation in larger prospective studies.
системний червоний вовчак; тестостерон; гіпогонадизм; чоловіки; глюкокортикоїди; протеїнурія
systemic lupus erythematosus; testosterone; hypogonadism; men; glucocorticoids; proteinuria
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Protsenko HO, Dubas VV. Systemic lupus erythematosus: the state of the problem in Ukraine and the world. Ukr J Rheumatol. 2020;4(82):25-34. https://doi.org/10.32471/rheumatology.2707-6970.82.15749. Ukrainian.
- Christou EAA, Banos A, Kosmara D, Bertsias GK, Boum–pas DT. Sexual dimorphism in SLE: above and beyond sex hormones. Lupus. 2019 Jan;28(1):3-10. doi: 10.1177/0961203318815768.
- Cutolo M, Straub RH. Sex steroids and autoimmune rheumatic diseases: state of the art. Nat Rev Rheumatol. 2020;16(11):628-644. doi: 10.1038/s41584-020-0503-4.
- Holovach IYu, Yehudina YeD, Ter-Vartanyan SH. Advances in diagnosis, pathogenesis and treatment of neuropsychiatric systemic lupus erythematosus: literature review 2017-2019. Ukrainian Journal of Rheumatology. 2020;3(81):33-41. doi: 10.32471/rheumatology.2707-6970.81.15518. Ukrainian.
- Rekalov DH, Daniuk IO. Non-Hodgkin’s lymphoma in patients with systemic lupus erythematosus: problems of diagnosis on the example of a clinical case. Ukrainian Journal of Rheumatology. 2023;2(92):58-61. doi: 10.32471/rheumatology.2707-6970.92.17843. Ukrainian.
- Folomeev M, Kosheleva N, Alekberova Z. Systemic lupus erythematosus associated with Klinefelter’s syndrome: a case report from the USSR. J Rheumatol. 1991 Jun;18(6):940-1. PMID: 1895282.
- Lavalle C, Loyo E, Paniagua R, Bermudez JA, Herrera J, Graef A, et al. Correlation study between prolactin and androgens in male patients with systemic lupus erythematosus. J Rheumatol. 1987 Apr;14(2):268-72.
- Horpynchenko II, Hurzhenko YuM, Spyrydonenko VV. Male hypogonadism (according to the materials of the European Association of Urology). Health of Man. 2022;4(83):5-23. https://doi.org/10.30841/2307-5090.4.2022.274432. Ukrainian.
- Baillargeon J, Al Snih S, Raji MA, Urban RJ, Sharma G, Sheffield-Moore M, et al. Hypogonadism and the risk of rheumatic autoimmune disease. Clin Rheumatol. 2016 Dec;35(12):2983-2987. doi: 10.1007/s10067-016-3330-x.
- Malkin CJ, Pugh PJ, Jones RD, Kapoor D, Channer KS, Jones TH. The effect of testosterone replacement on endogenous inflammatory cytokines and lipid profiles in hypogonadal men. J Clin Endocrinol Metab. 2004 Jul;89(7):3313-8. doi: 10.1210/jc.2003-031069.
- Cutolo M, Sulli A, Capellino S, Villaggio B, Montagna P, Pizzorni C, et al. Anti-TNF and sex hormones. Ann N Y Acad Sci. 2006 Jun;1069:391-400. doi: 10.1196/annals.1351.037.
- Savchenko L, Mykytiuk M, Cinato M, Tronchere H, Kunduzova O, Kaidashev I. IL-26 in the induced sputum is associated with the level of systemic inflammation, lung functions and body weight in COPD patients. Int J Chron Obstruct Pulmon Dis. 2018;13:2569-2575. doi: 10.2147/COPD.S164833.
- Inman RD, Jovanovic L, Markenson JA, Longcope C, Dawood MY, Lockshin MD. Systemic lupus erythematosus in men. Genetic and endocrine features. Arch Intern Med. 1982 Oct;142(10):1813-5.
- Stahl NI, Decker JL. Androgenic status of males with systemic lupus erythematosus. Arthritis Rheum. 1978 Jul-Aug;21(6):665-8. doi: 10.1002/art.1780210609. PMID: 736997.
- Arnaud L, Nordin A, Lundholm H, Svenungsson E, Hellbacher E, Wikner J, et al. Effect of Corticosteroids and Cyclophosphamide on Sex Hormone Profiles in Male Patients With Systemic Lupus Erythematosus or Systemic Sclerosis. Arthritis Rheumatol. 2017 Jun;69(6):1272-1279. doi: 10.1002/art.40057.
- Miller MH, Urowitz MB, Gladman DD, Killinger DW. Systemic lupus erythematosus in males. Medicine (Baltimore). 1983 Sep;62(5):327-34. doi: 10.1097/00005792-198309000-00005.
- Masala A, Faedda R, Alagna S, Satta A, Chiarelli G, Rovasio PP, et al. Use of testosterone to prevent cyclophosphamide-induced azoospermia. Ann Intern Med. 1997 Feb 15;126(4):292-5. doi: 10.7326/0003-4819-126-4-199702150-00005.
- Mok CC, Lau CS. Profile of sex hormones in male patients with systemic lupus erythematosus. Lupus. 2000;9(4):252-7. doi: 10.1191/096120300680198926.
- Folomeev M, Dougados M, Beaune J, Kouyoumdjian JC, Nahoul K, Amor B, et al. Plasma sex hormones and aromatase activity in tissues of patients with systemic lupus erythematosus. Lupus. 1992 May;1(3):191-5. doi: 10.1177/096120339200100312.
- Zheng Z, Pan J, Liu M, Chen Z, Zhang L, Gao J, et al. Anemia and testosterone deficiency risk: insights from NHANES data analysis and a Mendelian randomization analysis. Aging Male. 2024 Dec;27(1):2346312. doi: 10.1080/13685538.2024.2346312.
- Stepaniuk TV, Shevchuk SV. The state of the psycho-emotio–nal sphere in patients with systemic lupus erythematosus, the relationship with the course of the disease. Ukrainian Journal of Rheumatology. 2024;2(96):31-38. doi: 10.32471/rheumatology.2707-6970.96.18908. Ukrainian.
- Rekalov DH, Daniuk IO. Lungs and systemic lupus erythemato: a clinical case of the effective use of nintedanib in the treatment of common interstitial lupus pneumonia. Ukrainian Journal of Rheumatology. 2024;2(96):26-30. doi: 10.32471/rheumatology.2707-6970.96.18984. Ukrainian.
- Pankiv V, Yuzvenko T, Kobyliak N, Pankiv I. Correction of Androgen Deficiency in Men with Type 2 Diabetes. Rev Recent Clin Trials. 2022;17(1):34-39. doi: 10.2174/1574887116666211202155304. PMID: 34856912.
- De Silva NL, Papanikolaou N, Grossmann M, Antonio L, Quinton R, et al. Male hypogonadism: pathogenesis, diagnosis, and mana–gement. Lancet Diabetes Endocrinol. 2024 Oct;12(10):761-774. doi: 10.1016/S2213-8587(24)00199-2. Epub 2024 Aug 16. PMID: 39159641.