
Международный эндокринологический журнал Том 22, №4, 2026
Вернуться к номеру
Протизапальний засіб для корекції розладів вуглеводного та ліпідного обміну при панкреатогенному цукровому діабеті за коморбідного перебігу хронічного панкреатиту і хронічного обструктивного захворювання легень
Авторы: O.S. Khukhlina (1), I.V. Dudka (1), O.O. Abrahamovych (2), T.V. Dudka (1)
(1) - Bukovinian State Medical University, Chernivtsi, Ukraine
(2) - Danylo Halytsky Lviv National Medical University, Lviv, Ukraine
Рубрики: Эндокринология
Разделы: Клинические исследования
Версия для печати
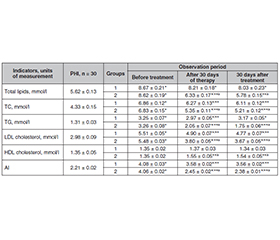
Актуальність. Стрімке зростання частоти поєднаного перебігу хронічного панкреатиту (ХП), панкреатогенного цукрового діабету (ПЦД) та хронічного обструктивного захворювання легень (ХОЗЛ) пояснюється наявністю фундаментальних механізмів взаємного обтяження. ХП і ХОЗЛ виступають детермінантами глибоких розладів вуглеводного й жирового обмінів, оскільки і підшлункова залоза, і легенева тканина відіграють стратегічну роль у системній метаболічній регуляції. Мета: провести комплексну оцінку параметрів глікемічного статусу, механізмів регуляції метаболізму вуглеводів та ліпідного профілю сироватки крові в пацієнтів із загостренням ХП, що перебігає на тлі коморбідних станів (ХОЗЛ та ПЦД), у динаміці лікування із включенням препарату з гепато- та панкреатопротекторною дією до схеми стандартної терапії. Матеріали та методи. Проведено аналіз ефективності лікування осіб із діагнозом ХП, ускладненим ПЦД та супутнім ХОЗЛ. Контрольна група (перша, n = 48) отримувала виключно базисну терапію, що відповідала протоколам лікування ХП, ХОЗЛ і ПЦД. Основна група (друга, n = 45) на додаток до ідентичного базисного лікування приймала препарат із гепато- та панкреатопротекторною дією. Результати. Встановлено, що при додаванні до схеми лікування препарату з гепато- та панкреатопротекторними ефектами у хворих другої групи на 30-й день терапії у 2,5 раза знизився рівень постпрандіальної глюкози (у першій — в 1,3 раза), концентрація ендогенного інсуліну зросла в 1,6 раза (у першій групі — невірогідно), глюкагону — у 4,7 раза (у першій групі — в 1,2 раза), індекс HOMA-B — у 6,6 раза (у першій групі — в 1,5 раза). Аналіз показників ліпідограми показує, що на 30-й день лікування у другій групі хворих вміст холестеролу знизився на 21,7 % (у першій групі — на 8,6 %), трацилгліцеролів — на 37,1 % (у першій групі — на 8,6 %), ХС ЛПНЩ — на 36,7 % (у першій групі — на 11,1 %), рівень ХС ЛПВЩ зріс на 14,8 % (у першій групі — не змінився), індекс атерогенності знизився на 39,7 % (у першій групі — на 12,3 %). Перелічені зміни зберігали позитивну динаміку через 30 днів після закінчення лікування. Висновки. Включення препарату з гепато- та панкреатопротекторними ефектами до комплексної терапії ХП, ПЦД та ХОЗЛ забезпечує вірогідну стабілізацію глікемічного профілю, демонструє потужну ліпідкоригувальну дію, дозволяє досягти ремісії та стабілізації метаболічних показників, які зберігаються протягом щонайменше одного місяця після завершення курсу лікування.
Background. The rapid increase in the frequency of the combined course of chronic pancreatitis (CP), pancreatogenic diabetes mellitus (PDM) and chronic obstructive pulmonary disease (COPD) is explained by the presence of fundamental mechanisms of mutual aggravation. CP and COPD are determinants of profound disorders of carbohydrate and lipid metabolism, since both the pancreas and lung tissue play a strategic role in systemic metabolic regulation. The purpose of this study was to conduct a comprehensive assessment of the parameters of glycemic status, mechanisms of carbohydrate metabolism regulation and serum lipid profile in patients with exacerbation of CP, occurring against the background of comorbid conditions (COPD and PDM) in the dynamics of treatment with the inclusion of the drug with hepatoprotective and pancreatoprotective effects in the standard therapy regimen. Materials and methods. The analysis on the effectiveness of treatment of patients with a diagnosis of CP complicated by PDM and with concomitant COPD was conducted. The control group (group 1, n = 48) received only basic therapy, which corresponded to the treatment protocols for CP, COPD and PDM. The main group (group 2, n = 45) in addition to the identical basic treatment took the drug with hepatoprotective and pancreatoprotective effects. Results. The study founded that when the hepato- and pancreaticoprotector was added to the treatment regimen on the 30th day of therapy, the postprandial glucose level in patients of group 2 decreased by 2.5 times (in group 1, by 1.3 times), the concentration of endogenous insulin increased by 1.6 times (in group 1, improbable), the glucagon level by 4.7 times (in group 1, by 1.2 times), and the HOMA-B index by 6.6 times (in group 1, by 1.5 times). Analysis of lipid profile indicators shows that on the 30th day of treatment in group 2 patients, the cholesterol content decreased by 21.7 % (in group 1, by 8.6 %), triacylglycerols by 37.1 % (in group 1, by 8.6 %), the low-density lipoprotein cholesterol by 36.7 % (in group 1, by 11.1 %), the high-density lipoprotein cholesterol level increased by 14.8 % (in group 1, it did not change), and atherogenic index decreased by 39.7 % (in group 1, by 12.3 %). The listed changes maintained positive dynamics 30 days after the end of treatment. Conclusions. Including the drug with hepatoprotective and pancreatoprotective effects in the comprehensive therapy of CP, PDM and COPD provides reliable stabilization of the glycemic profile, demonstrates a powerful lipid-correcting effect, allows achieving remission and stabilization of metabolic indicators, which are maintained for at least one month after the completion of the treatment course.
хронічний панкреатит; хронічне обструктивне захворювання легень; панкреатогенний цукровий діабет; ліпіди; обмін вуглеводів
chronic pancreatitis; chronic obstructive pulmonary disease; pancreatogenic diabetes mellitus; lipids; carbohydrate metabolism
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Dudka I, Khukhlina O, Dudka T, Voyevidka O, Roshchuk O. Рeculiarities of formation of carbohydrate metabolism disorders with comorbid chronic pancreatitis and chronic obstructive pulmonary disease. Wiad Lek. 2023;76(7):1586-1593. doi: 10.36740/WLek202307111.
- Ghafil NY, Dananah FM, Hassan ES, Alkaabi YSA. Comorbidities in patients with chronic obstructive pulmonary disease: a comprehensive study. J Med Life. 2023;16(7):1013-1016. doi: 10.25122/jml-2022-0057.
- Göltl P, Murillo K, Simsek O, Wekerle M, Ebert MP, et al. Impact of alcohol and smoking cessation on the course of chronic pancreatitis. Alcohol. 2024;119:29-35. doi: 10.1016/j.alcohol.2023.11.006.
- Dudka IV. Changes in particular indicators of the glycemic profile in patients with chronic pancreatitis with accompanying chronic obstructive pulmonary disease. Actual Problems of Modern Medicine: Bulletin of Ukrainian Medical Stomatological Academy. 2025;25(1):4-10. doi: 10.31718/2077-1096.25.1.4 (in Ukrainian).
- Khukhlina OS, Dudka IV. Effect of Antral on the intensity of systemic inflammation and fibrosis of the pancreas in chronic pancreatitis with comorbidity with chronic obstructive pulmonary disease in the exacerbation phase. Herald of Pancreatic Club. 2025;3:39-46. doi: 10.33149/vkp.2025.03.06 (in Ukrainian).
- Figueira Gonçalves JM, García Bello MÁ, Golpe R, Alonso Jerez JL, García-Talavera I. Impact of diabetes mellitus on the risk of severe exacerbation in patients with chronic obstructive pulmonary disease. Clin Respir J. 2020;14(12):1208-1211. doi: 10.1111/crj.13255.
- Liu W, Qiao Z, Du C, Zhang X. Comprehensive age-period-cohort analysis of global pancreatitis burden and socioeconomic disparities (1990–2021). BMC Gastroenterol. 2025;25(1):630. doi: 10.1186/s12876-025-04222-1.
- Tsomidis I, Voumvouraki A, Kouroumalis E. The Pathogenesis of Pancreatitis and the Role of Autophagy. Gastroenterology Insights. 2024;15(2):303-341. doi: 10.3390/gastroent15020022.
- Ma Y, Yang X, Chatterjee V, Wu MH, Yuan SY. The gut-lung axis in systemic inflammation. Role of mesenteric lymph as a conduit. Am J Respir Cell Mol Biol. 2021;64(1):19-28. doi: 10.1165/rcmb.2020-0196TR.
- Bhattamisra SK, Siang TC, Rong CY, Annan NC, Sean EHY, et al. Type-3c Diabetes Mellitus, Diabetes of Exocrine Pancreas — An Update. Curr Diabetes Rev. 2019;15(5):382-394. doi: 10.2174/1573399815666190115145702.
- Dominguez-Muñoz JE, Vujasinovic M, de la Iglesia D, Cahen D, Capurso G, et al. European PEI Multidisciplinary Group. European guidelines for the diagnosis and treatment of pancreatic exocrine insufficiency: UEG, EPC, EDS, ESPEN, ESPGHAN, ESDO, and ESPCG evidence-based recommendations. United European Gastroenterol J. 2025;13(1):125-172. doi: 10.1002/ueg2.12674.
- Khalili D, Khayamzadeh M, Kohansal K, Ahanchi NS, Hashe–minia M, et al. Are HOMA-IR and HOMA-B good predictors for diabetes and pre-diabetes subtypes? BMC Endocr Disord. 2023;23(1):39. doi: 10.1186/s12902-023-01291-9.
- Li L, Zhang Y, Leng J, Li S, Lei Y, et al. The global, regional and national burden of pancreatitis due to alcohol use: results from the global burden of disease study 2021 and projections to 2040. PLoS One. 2025;20(7):e0327831. doi: 10.1371/journal.pone.0327831.
- Wayne CD, Benbetka C, Besner GE, Narayanan S. Challen–ges of managing type 3c diabetes in the context of pancreatic resection, cancer and trauma. J Clin Med. 2024;13(10):2993. doi:10.3390/jcm13102993.
- Ode KL, Imai Y, Norris AW. Approach to the patient with pancreatogenic diabetes. J Clin Endocrinol Metab. 2026;111(2):e569-e576. doi: 10.1210/clinem/dgaf623.
- Al Balushi H, Ahmed J, Ahuja LK, Barkha F, Shafeeq MI, et al. Evaluating the efficacy of antioxidant therapy in enhancing the quality of life of chronic pancreatitis patients: a systematic review. Cureus. 2024;16(4):e57402. doi: 10.7759/cureus.57402.
- Lin Z, Pandol S, Apte M, Jiang Y. Navigating chronic pancreatitis pain: a pathophysiological and therapeutic overview. Front Physiol. 2025;16:1622845. doi: 10.3389/fphys.2025.1622845.
- Swentek L, Chung D, Ichii H. Antioxidant Therapy in Pancreatitis. Antioxidants (Basel). 2021;10(5):657. doi: 10.3390/antiox10050657.
- Lytkin D, Tovchiga O, Udovitskiy V, Barbukho O. Efficacy of the coordinative compound of aluminium and N-(2,3-dimethylphenyl)-anthranilic (mefenamic) acid on the model of chronic alcohol-induced pancreatitis. Research Journal of Pharmacy and Techno–logy. 2024; 17(6):2531-2540. doi: 10.52711/0974-360X.2024.00396.
- Order of the Ministry of Health of Ukraine No. 638 dated September 10, 2014 “Unified clinical protocol of primary, secondary (specialized) medical care and medical rehabilitation “Chronic pancreatitis” (in Ukrainian). Available from: https://surl.li/eblwwt.
- Order of the Ministry of Health of Ukraine No. 1204 of July 4, 2023 “On approval of the Unified clinical protocol of primary and specialized medical care “Chronic pancreatitis” (in Ukrainian). Available from: https://surl.li/sledrg.
- Adapted evidence-based clinical guideline “Chronic obstructive pulmonary disease”. Kyiv: National Academy of Medical Sciences of Ukraine; 2020. 69 p. (in Ukrainian). Available from: https://surl.li/ssoecw.
- GOLD 2022 report “Global strategy for diagnosis, management, and prevention of chronic obstructive pulmonary disease (COPD)” 2023. Available from: https://goldcopd.org/2023-gold-report-2/.
- Order of the Ministry of Health of Ukraine No. 1118 dated 21.12.2012 “On the approval and implementation of medical and technological documents on the standardization of medical care for type 2 diabetes mellitus” (in Ukrainian). Available from: https://surl.li/eqrkxj.
- Unified clinical protocol for primary, emergency, secondary (specialized) and tertiary (highly specialized) medical care: type 1 diabetes mellitus in young people and adults, approved by Order of the Ministry of Health of Ukraine dated December 29, 2014, No. 1021 (in Ukrainian). Available from: https://surl.li/ieogpe.