
Журнал «Медицина неотложных состояний» Том 22, №4, 2026
Вернуться к номеру
Оцінка крихкості пацієнта на етапі доопераційної підготовки як важливий метод стратифікації з метою поліпшення результатів втручання
Авторы: Гарбар М.О. , Матолінець Н.В., Ушневич Ж.О., Світлик Г.В., Яремкевич Р.В.
ДНТ «Львівський національний медичний університет імені Данила Галицького», м. Львів, Україна
Рубрики: Медицина неотложных состояний
Разделы: Клинические исследования
Версия для печати
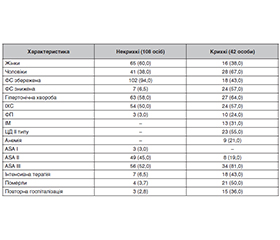
Актуальність. Стратифікація ризику пацієнта старшого віку та вибір хірургічної стратегії здійснюються з урахуванням крихкості, що є незалежним фактором ризику несприятливих подій після несерцевої хірургії. Комплексна підготовка до операційних втручань пацієнта із крихкістю входить у програму преабілітації, що активно впроваджується в сучасну світову практику. Мета: проаналізувати показник крихкості у пацієнтів із супутньою серцево-судинною патологією, яким проведені планові некардіальні операції, оцінити взаємозв’язок крихкості з клінічними характеристиками, результатами інструментальних та лабораторних обстежень, перебігом періопераційного періоду, лікарняною смертністю. Оцінити значення крихкості для доопераційної стратифікації з метою поліпшення післяопераційного періоду. Матеріали та методи. Ступінь крихкості доопераційно визначено 150 пацієнтам, які перенесли планову некардіохірургічну операцію та мали супутню серцево-судинну патологію. Проаналізовано функціональну здатність, фізичний статус за ASA, клінічні фактори ризику, результати сонографії серця, динаміку 12-канальної ЕКГ, показники загальноклінічного та біохімічного аналізів крові, визначено рівень NT-proBNP. Для оцінки крихкості використано клінічну шкалу крихкості. Результати. Крихкість встановлена у 28 % пацієнтів. Дві третини з них були чоловіками. У пацієнтів із крихкістю була нижча функціональна спроможність. Вони мали більше супутніх захворювань (цукровий діабет, анемія, серцево-судинні хвороби, вищий рівень креатиніну, трансаміназ) та вищий показник індексу серцевого ризику (RCRI). Більшість із них (81 %) належали до класу ASA III. Для крихких пацієнтів типовими були ознаки дисфункції (зниження фракції викиду, підвищення індексу Теі, вкорочення часу викиду в аорту, порушення діастолічного розслаблення) та ремоделювання (зміна геометрії) лівого шлуночка. У них виявлено вірогідно вищі значення натрійуретичного пептиду та середньої ЧСС, тенденцію до подовження інтервалу QT. Крихкі пацієнти довше перебували у стаціонарі, 43 % потребували інтенсивної терапії в післяопераційному періоді (на противагу 6,5 % пацієнтів без крихкості). Більше третини з них були повторно госпіталізовані протягом періоду спостереження. Половина осіб із крихкістю померли (у групі без крихкості — 3,7 %), серед них 75 % на стаціонарному етапі, середній час до смерті становив 23,67 ± 2,44 дня. Висновки. Крихкість асоціюється зі зниженням функціональної спроможності, коморбідністю, вищим ризиком анестезії, потребою в інтенсивній терапії, довшим перебуванням у стаціонарі, підвищеною летальністю. Клінічна шкала крихкості є доступним та надійним діагностичним тестом стратифікації пацієнтів з метою оптимізації та поліпшення післяопераційного відновлення, результатів операції та якості надання медичної допомоги.
Background. Risk stratification in elderly patients and the choice of surgical strategy are performed with consideration of frailty, which is an independent risk factor for adverse outcomes after non-cardiac surgery. Comprehensive preoperative preparation of frail patients is part of prehabilitation programs that are actively being implemented in modern medical practice. Goals of study was to analyze the level of frailty in patients with concomitant cardiovascular disease undergoing elective non-cardiac surgery; to assess the relationship between frailty and clinical characteristics, instrumental and laboratory findings, perioperative course, and in-hospital mortality; consequently, to evaluate the role of frailty in preoperative risk stratification to improve postoperative outcomes. Materials and methods. Frailty was assessed preoperatively in 150 patients who underwent elective non-cardiac surgery and had concomitant cardiovascular pathology. Functional capacity, physical status according to the ASA classification, clinical risk factors, echocardiographic findings, 12-lead ECG dynamics, general clinical and biochemical blood parameters, and NT-proBNP levels were analyzed. Frailty was evaluated using the Clinical Frailty Scale. Results. Frailty was identified in 28 % of patients, two-thirds of whom were male. Frail patients demonstrated lower functional capacity and had a higher burden of comorbidities (diabetes mellitus, anemia, cardiovascular diseases, higher creatinine and transaminase levels) as well as a higher Revised Cardiac Risk Index. Most of them (81 %) were classified as ASA III. Frail patients commonly exhibited signs of left ventricular dysfunction (reduced ejection fraction, increased Tei index, shortened aortic ejection time, impaired diastolic relaxation) and remodeling (changes in geometry). They also had significantly higher levels of natriuretic peptide, higher mean heart rate, and a tendency toward QT interval prolongation. Frail patients had longer hospital stays, and 43 % required postoperative intensive care (compared to 6.5 % of non-frail patients). More than one-third were rehospitalized during the follow-up period. Half of the frail patients died (compared to 3.7 % in the non-frail group), with 75 % of deaths occurring during hospitalization; the mean time to death was 23.67 ± 2.44 days. Conclusions. Frailty is associated with reduced functional capacity, higher comorbidity burden, increased anesthetic risk, greater need for intensive care, longer hospital stay, and higher mortality. The Clinical Frailty Scale is an accessible and reliable tool for patient stratification, aimed at optimizing postoperative recovery, improving surgical outcomes, and enhancing the quality of medical care.
некардіальні хірургічні втручання; періопераційний період; крихкість; мультимодальна преабілітація
non-cardiac surgical interventions; perioperative period; frailty; multimodal prehabilitation
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Aldecoa C, Bettelli G, Bilotta F, et al. Update of the European Society of Anaesthesiology and Intensive Care Medicine evidence-based and consensus-based guideline on postoperative delirium in adult patients. Eur J Anaesthesiol. 2024;41:81-108. doi: 10.1097/EJA.0000000000001876.
- Thompson A, Fleischmann KE, Smilowitz NR, et al. 2024 AHA/ACC/ACS/ASNC/HRS/SCA/SCCT/SCMR/SVM Guidelines for Perioperative Cardiovascular Management for Noncardiac Surgery: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2024;150(19):e351-e442. doi: 10.1161/CIR.0000000000001285.
- Lamperti M, Romero CS, Guarracino F, et al. Preoperative assessment of adults undergoing elective noncardiac surgery. Updated guidelines from the European Society of Anaesthesiology and Intensive Care. Eur J Anaesthesiol. 2025;42:1-35. doi: 10.1097/EJA.0000000000002069.
- Siddiqui E, Banco D, Berger JS, et al. Frailty assessment and perioperative major adverse cardiovascular events after noncardiac surgery. Am J Med. 2023;136:372-379.e375. doi: 10.1016/j.amjmed.2022.12.033.
- Hall DE, Arya S, Schmid KK, et al. Association of a frailty screening initiative with postoperative survival at 30, 180, and 365 days. JAMA Surg. 2017;152:233-240. doi: 10.1001/jamasurg.2016.4219.
- Birkelbach O, Morgeli R, Spies C, et al. Routine frailty assessment predicts postoperative complications in elderly patients across surgical disciplines — a retrospective observational study. BMC Anesthesiol. 2019;19:204. doi: 10.1186/s12871-019-0880-x.
- Tjeertes EKM, van Fessem JMK, Mattace-Raso FUS, et al. Influence of frailty on outcome in older patients undergoing non-cardiac surgery — a systematic review and meta-analysis. Aging Dis. 2020;11:1276-1290. doi: 10.14336/AD.2019.1024.
- Lin HS, Watts JN, Peel NM, et al. Frailty and postoperative outcomes in older surgical patients: a systematic review. BMC Geriatr. 2016;16:157. doi: 10.1186/s12877-016-0329-8.
- Aucoin SD, Hao M, Sohi R, et al. Accuracy and feasibility of clinically applied frailty instruments before surgery: a systematic review and metaanalysis. Anesthesiology. 2020;133:78-95. doi: 10.1097/ALN.0000000000003257.
- McIsaac DI, Harris EP, Hladkowicz E, et al. Prospective comparison of preoperative predictive performance between 3 leading frailty instruments. Anesth Analg. 2020;131:263-272. doi: 10.1213/ANE.0000000000004475.
- Rabelo LG, Bjornsdottir A, Jonsdottir AB, et al. Frailty assessment tools and associated postoperative outcomes in older patients undergoing elective surgery: a prospective pilot study. Acta Anaesthesiol Scand. 2023;67:150-158. doi: 10.1111/aas.14162.
- Rockwood K, Theou O. Using the Clinical Frailty Scale in Allocating Scarce Health Care Resources. Can Geriatr J. 2020;23(3):210-215. doi: 10.5770/cgj.23.463.
- Shulman MA, Wallace S, Gilbert A, et al. Predicting death or disability after surgery in the older adult. Anesthesiology. 2023;139:420-431. doi: 10.1097/ALN.0000000000004683.
- Optimal Perioperative Management of the Geriatric Patient: A Best Practices Guideline from the American College of Surgeons NSQIP and the American Geriatrics Society. Journal of the American College of Surgeons. 2016;222(5):930-947. doi: 10.1016/j.jamcollsurg.2015.12.026.
- Alvarez-Nebreda ML, Bentov N, Urman RD, Setia S, Huang JC, Pfeifer K, et al. Recommendations for preoperative ma–nagement of frailty from the Society for Perioperative Assessment and Quality Improvement (SPAQI). J Clin Anesth. 2018;47:33-42. doi: 10.1016/j.jclinane.2018.02.011.
- Nidadavolu LS, Ehrlich AL, Sieber FE, et al. Preoperative evaluation of the frail patient. Anesth Analg. 2020;130:1493-1503. doi: 10.1213/ANE.0000000000004735.
- Norris CM, Close JCT. Prehabilitation for the frailty syndrome: improving outcomes for our most vulnerable patients. Anesth Analg. 2020;130:1524-1533. doi: 10.1213/ANE.0000000000004785.
- Charipova K, Urits I, Viswanath O, et al. Preoperative assessment and optimization of cognitive dysfunction and frailty in the ambulatory surgical patient. Curr Opin Anaesthesiol. 2020;33:732-739. doi: 10.1097/ACO.0000000000000901.
- Walston J, Buta B, Xue QL. Frailty screening and interventions: considerations for clinical practice. Clin Geriatr Med. 2018;34:25-38. doi: 10.1016/j.cger.2017.09.004.
- Richter D, Guasti L, Walker D, et al. Frailty in cardiology: definition, assessment and clinical implications for general cardiology. A consensus document of the Council for Cardiology Practice (CCP), Association for Acute Cardio Vascular Care (ACVC), Association of Cardiovascular Nursing and Allied Professions (ACNAP), European Association of Preventive Cardiology (EAPC), European Heart Rhythm Association (EHRA), Council on Valvular Heart Diseases (VHD), Council on Hypertension (CHT), Council of Cardio-Oncology (CCO), Working Group (WG) Aorta and Peripheral Vascular Diseases, WG e-Cardiology, WG Thrombosis, of the European Society of Cardiology, European Primary Care Cardiology Society (EPCCS). Eur J Prev Cardiol. 2022;29:216-227. doi: 10.1093/eurjpc/zwaa167.
- Brendon HR, James DC, Holly AC, et al. Physiological relationship between cardiorespiratory fitness and fitness for surgery: a narrative review. Br J Anaesth. 2023;130(2):122-132. doi: 10.1016/j.bja.2022.10.039.
- Charlotte JLM, Enrico MM, Miquel C-M, et al. Effect of Multimodal Prehabilitation on Reducing Postoperative Complications and Enhancing Functional Capacity Following Colorectal Cancer Surgery: The PREHAB Randomized Clinical Trial. JAMA Surg. 2023;158(6):572-581. doi: 10.1001/jamasurg.2023.0198.
- Lurati BG, Puelacher Ch, Menosi GD, et al. Association between self-reported functional capacity and major adverse cardiac events in patients at elevated risk undergoing noncardiac surgery: a prospective diagnostic cohort study. Br J Anaesth. 2020;126:102-110. doi: 10.1016/j.bja.2020.08.041.
- Duke Activity Status Index (DASI). Available from: https://www.mdcalc.com/calc/3910/duke-activity-status-index-dasi.
- Statement on ASA Physical Status Classification System. Available from: www.asahq.org/standards-and-practice-parameters/statement-on-asa-physical-status-classification-system. Accessed: December 13, 2020.
- Ford MK, Beattie WS, Wijeysundera DN. Systematic review: prediction of perioperative cardiac complications and mortality by the Revised Cardiac Risk Index. Ann Intern Med. 2010;152:26-35. doi: 10.7326/0003-4819-152-1-201001050-00007.
- Lancellotti P, Cosyns B. The EACVI Echo Handbook. The European Society of Cardiology Series. OXFORD University Press. 2016. 588 p.
- Гарбар М.О., Матолінець Н.В., Ястремська О.О., Світлик Г.В. Серцеві біомаркери як важливий компонент періопераційного менеджменту пацієнта із супутньою серцевою патологією. Медицина невідкладних станів. 2025;21(8):22-31. doi: http://dx.doi.org/10.22141/2224-0586.21.8.2025.1947.
- Collard RM, Boter H, Schoevers RA, et al. Prevalence of frailty in community-dwelling older persons: a systematic review. J Am Geriatr Soc. 2012;60:1487-1492. doi: 10.1111/j.1532-5415.2012.04054.x.
- Захворювання серцево-судинної системи: фактори ризику та профілактика. Available from: https://moz.gov.ua/uk/zahvorjuvannja-sercevo-sudinnoi-sistemi-faktori-riziku-ta-profilaktika.
- Здоров’я та тривалість життя українців напряму залежить від чистого довкілля. Available from: https://www.kmu.gov.ua/news/mindovkillya-zdorovya-ta-trivalist-zhittya-ukrayinciv-napryamu-zalezhit-vid-chistogo-dovkillya.
- Denfeld QE, Winters-Stone K, Mudd JO, et al. The prevalence of frailty in heart failure: a systematic review and meta-analysis. Int J Cardiol. 2017;236:283-289. doi: 10.1016/j.ijcard.2017.01.153.
- Uchmanowicz I, Lee CS, Vitale C, et al. Frailty and the risk of all-cause mortality and hospitalization in chronic heart failure: a meta-analysis. ESC Heart Fail. 2020;7:3427-3437. doi: 10.1002/ehf2.12827.
- Mirna M, Schmutzler L, Vogl F, et al. Tei Index Is a Useful Adjunctive Tool in the Diagnostic Workup of Patients with Acute Myocarditis. J Cardiovasc Dev Dis. 2022;9(8):283. doi: 10.3390/jcdd9080283.
- Mansour H, Nassar AI, Abdel R, et al. Can Tei Index Predict High Syntax Score in Patients with Chronic Coronary Syndrome and Normal Left Ventricular Systolic Function? Journal of Cardiovascular Echography. 2021;31(1):11-16. doi: 10.4103/jcecho.jcecho_73_20.
- Shu N, Yuma N, Masayuki Y, et al. Plasma brain natriuretic peptide level in older outpatients with heart failure is associated with physical frailty, especially with the slowness domain. J Geriatr Cardiol. 2016;13(7):608-614. doi: 10.11909/j.issn.1671-5411.2016.07.014.
- Prokopidis K, Ishiguchi H, Jordan C, et al. Association between natriuretic peptides and C-reactive protein with frailty in heart failure: a systematic review and meta-analysis Aging Clin Exp Res. 2024 Mar 6;36(1):57. doi: 10.1007/s40520-024-02713-x.
- Qi Zh, Rui Zh, Yi-Ning H, et al. Frailty and risk of metabolic dysfunction-associated steatotic liver disease and other chronic liver diseases. Journal of Hepatology. 2025;82(3),427-437. doi: 10.1016/j.jhep.2024.08.024.
- Xiaotian S, Shan W, Jieqiong H, Fei C. Relationship of Frailty with Kidney Function in Adults More Than 60-Years-Old: Effect of Using Different Formulas to Estimate Glomerular Filtration Rate. Clin Іnterv Aging. 2023;18:999-1007. doi: 10.2147/CIA.S409140.
- Nair D, Liu ChK, Raslan R. Frailty in Kidney Disease: A Comprehensive Review to Advance Its Clinical and Research Applications. American Journal of Kidney Diseases. 2025;85(1):89-103. doi: 10.1053/j.ajkd.2024.04.018.
- Pecorelli N, Guarneri G, Di Salvo F, et al. The Impact of Postoperative Complications on Recovery of Health-Related Quality of Life and Functional Capacity After Pancreatectomy: Findings from a Prospective Observational Study. Ann Surg. 2024;280(5):719-727. doi: 10.1097/SLA.0000000000006472.
- Pearse RM, Moreno RP, Bauer P, et al. Mortality after surgery in Europe: a 7 day cohort study. Lancet. 2012;380:1059-1065. doi: 10.1161/CIRCHEARTFAILURE.121.009427.
- Martins RS, Chang Y-H, Etzioni D, et al. Understanding Variation in In-hospital Mortality After Major Surgery in the Uni–ted States. Annals of Surgery. 2023;278(6):865-872. doi: 10.1097/SLA.0000000000005862.