
Журнал «Медицина неотложных состояний» Том 22, №4, 2026
Вернуться к номеру
Взаємообтяжуючі ускладнення в розвитку гепаторенального синдрому при декомпенсованій портальній гіпертензії
Авторы: M.I. Tutchenko (1), D.M. Patrakh (1), D.V. Rudyk (1), M.S. Besedinskyi (1), A.V. Lovin (1), I.V. Klyuzko (2)
(1) - Bogomolets National Medical University, Kyiv, Ukraine
(2) - Vyshhorod Central District Hospital, Vyshhorod, Kyiv region, Ukraine
Рубрики: Медицина неотложных состояний
Разделы: Клинические исследования
Версия для печати
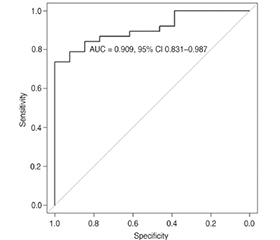
Актуальність. Гепаторенальний синдром (ГРС), що виникає при декомпенсованій портальній гіпертензії (ПГ), характеризується розвитком ниркової недостатності, зростанням рівня креатиніну крові, прогресуванням олігурії. У третини пацієнтів із цирозом печінки класу С за Child — Pugh розвивається ГРС. Мета: оптимізувати ранню діагностику й лікування, а також визначити фактори ризику розвитку ГРС і пов’язаної з ним летальності. Матеріали та методи. Проаналізовано 126 історій хвороб пацієнтів із декомпенсованою ПГ, яких лікували в КНП «Київська міська клінічна лікарня швидкої медичної допомоги» та на базі кафедри хірургії стоматологічного факультету НМУ імені О.О. Богомольця у 2022–2024 роках. ГРС виявлено в 51 (40,5 %) випадку. Критеріями встановлення діагнозу були підвищення рівня креатиніну > 150 мкмоль/л (1,69 мг/дл) або > 26,5 мкмоль/л (0,3 мг/дл) протягом 48 год за наявності олігурії без супутніх ознак ураження нирок, зокрема гематурії. Пацієнтів розподілено на дві групи. До першої групи увійшло 24 (47,1 %) особи, у яких ГРС та позагоспітальний спонтанний бактеріальний перитоніт (СБП) діагностовано впродовж першої доби і при проведенні гемотрансфузійної підтримки дотримувались рестриктивної тактики. До другої — 27 (52,9 %) хворих, у яких ГРС та нозокоміальний СБП встановлено на 3-тю — 5-ту добу лікування, а гемотрансфузійну підтримку виконували з дотриманням ліберальної тактики. Оцінено роль гемотрансфузійної підтримки, тяжкості асциту й СБП у формуванні ГРС як взаємообтяжуючих чинників. Результати. Аналіз отриманих даних показав, що поєднання великого асциту, СБП та ліберальної гемотрансфузійної тактики формує несприятливий прогностичний комплекс, пов’язаний зі значним підвищенням ризику смерті. Розвиток ГРС частіше асоціювався з великим асцитом (70,8 %), нозокоміальним СБП (37,0 %) та ліберальною гемотрансфузійною тактикою (52,9 %). Серед 126 обстежених пацієнтів прооперовано 27 (21,4 %), а ГРС у післяопераційному періоді розвинувся в 1 (4,2 %) хворого першої групи та у 2 (7,4 %) — другої. Загальна летальність становила 74,5 % (n = 38), у першій групі померло 14 (58,3 %) осіб, у другій — 24 (88,9 %), p = 0,03. За результатами ROC-аналізу модель продемонструвала високу прогностичну здатність щодо летальності (AUC = 0,909; 95% довірчий інтервал 0,831–0,987), що підтверджує її добру дискримінаційну силу для стратифікації ризику в пацієнтів із ГРС. Висновки. ГРС є тяжким ускладненням декомпенсованої ПГ із високою летальністю. Ліберальна трансфузійна тактика, виражений асцит і СБП підвищують ризик його розвитку та прогресування. Ранній моніторинг діурезу й рівня креатиніну є ключовим для своєчасної діагностики, профілактики та лікування ГРС.
Background. Hepatorenal syndrome (HRS) developing in the setting of decompensated portal hypertension (PH) is characterized by progressive renal failure, elevated serum creatinine levels, and worsening oliguria. HRS occurs in approximately one-third of patients with Child-Pugh class C liver cirrhosis. The purpose was to optimize early diagnosis and treatment, as well as to identify risk factors for the development of HRS and associated mortality. Materials and methods. A total of 126 medical records of patients with decompensated PH treated at the Kyiv City Emergency Hospital and the Department of Surgery, Dental Faculty, Bogomolets National Medical University, between 2022 and 2024 were analyzed. HRS was diagnosed in 51 (40.5 %) cases. Diagnostic criteria included an increase in serum creatinine > 150 µmol/L (1.69 mg/dL) or ≥ 26.5 µmol/L (0.3 mg/dL) within 48 hours in the presence of oliguria and absence of other signs of intrinsic renal injury, particularly hematuria. Patients were divided into two groups. The first group included 24 (47.1 %) patients in whom HRS and community-acquired spontaneous bacterial peritonitis (SBP) were diagnosed within the first 24 hours, and a restrictive transfusion strategy was applied. The second group comprised 27 (52.9 %) participants in whom HRS and nosocomial SBP were diagnosed on days 3–5 of hospitalization, and a liberal transfusion strategy was used. The impact of transfusion strategy, ascites severity, and SBP as mutually aggravating factors in HRS development was assessed. Results. Analysis showed that the combination of large-volume ascites, SBP, and a liberal transfusion strategy forms an unfavorable prognostic complex associated with a significantly increased risk of mortality. HRS development was more frequently associated with large-volume ascites (70.8 %), nosocomial SBP (37.0 %), and a liberal transfusion strategy (52.9 %). Among 126 patients, 27 (21.4 %) underwent surgery. In the postoperative period, HRS developed in 1 (4.2 %) patient in the first group and in 2 (7.4 %) patients in the second group. Overall mortality was 74.5 % (n = 38), with 14 deaths (58.3 %) in the first group and 24 (88.9 %) in the second group (p = 0.03). According to ROC analysis, the model demonstrated high predictive performance for mortality (AUC = 0.909; 95% CI 0.831–0.987), confirming strong discriminative ability for risk stratification in patients with HRS. Conclusions. HRS is a severe complication of decompensated PH associated with high mortality. A liberal transfusion strategy, severe ascites, and SBP increase the risk of its development and progression. Early monitoring of urine output and serum creatinine levels is critical for timely diagnosis, prevention, and management of HRS.
гепаторенальний синдром; цироз печінки; портальна гіпертензія; альбумін; варикозна кровотеча; креатинін; діурез; спонтанний бактеріальний перитоніт
hepatorenal syndrome; liver cirrhosis; portal hypertension; albumin; variceal bleeding; creatinine; diuresis; spontaneous bacterial peritonitis
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Bataller R, Ginés P, Guevara M, Arroyo V. Hepatorenal syndrome. Semin Liver Dis. 1997;17(3):233-247. doi: 10.1055/s-2007-1007201.
- Marchak K, Singh D, Barron MP, Trivedi P. Hepatorenal syndrome: updates on definition, classification, pathophysiology and treatment options. Tech Vasc Interv Radiol. 2025;28(4):101077. doi: 10.1016/j.tvir.2025.101077.
- Tutchenko MI, Patrakh DM. Hepatorenal syndrome: historical perspectives on the recognition of the problem. Gen Surg. 2026 Mar;(1):58. doi: 10.30978/GS-2026-1-58.
- Attieh RM, Wadei HM. Acute kidney injury in liver cirrhosis. Diagnostics (Basel). 2023;13(14):2361. doi: 10.3390/diagnostics13142361.
- Ozturk NB, Dinc EJ, Swami A, Gurakar A. Acute kidney injury and hepatorenal syndrome in patients with cirrhosis. J Clin Med. 2023;13(1):199. doi: 10.3390/jcm13010199.
- Braga QM, Schacher FC, Mattos AA, Mattos ÂZ. Terlipressin for the treatment of hepatorenal syndrome: a meta-analysis of rando–mized controlled trials. Eur J Gastroenterol Hepatol. 2025;37(6):753-760. doi: 10.1097/MEG.0000000000002954.
- Biggins SW, Angeli P, Garcia-Tsao G, Ginès P, Ling SC, Na–dim MK, et al. Diagnosis, evaluation, and management of ascites, spontaneous bacterial peritonitis and hepatorenal syndrome: 2021 practice guidance by the American Association for the Study of Liver Diseases. Hepatology. 2021;74(2):1014-1048. doi: 10.1002/hep.31884.
- Wong F. Management of refractory ascites. Clin Mol Hepatol. 2023;29(1):16-32. doi: 10.3350/cmh.2022.0104.
- Choi JC, Yoo JJ. Hepatorenal syndrome. Korean J Gastroenterol. 2023;82(5):224-232. doi: 10.4166/kjg.2023.108.
- Hamilton M. Hepatorenal syndrome treatment with terlipressin and albumin. Crit Care. 2000;2(1):6039. doi: 10.1186/ccf-2000-6039.
- Rudyk DV, Tutchenko MI, Chub SL, Besedinsky MS. Portal hypertension and emergency care. Wiad Lek. 2024;77(7):1485-1489. doi: 10.36740/WLek202407125.
- Kiani C, Zori AG. Recent advances in pathophysiology, diagnosis and management of hepatorenal syndrome: a review. World J Hepatol. 2023;15(6):741-754. doi: 10.4254/wjh.v15.i6.741.
- Serper M, Tang H, Zhang S, McCullough A, Kaplan DE, Taddei TH, et al. Clinical outcomes and care for spontaneous bacterial peritonitis: a national cohort study. Hepatology. 2025;82(5):1187-1197. doi: 10.1097/HEP.0000000000001251.
- Bai Z, Méndez-Sánchez N, Romeiro FG, Mancuso A, Phi–lips CA, Tacke F, et al. Use of albumin infusion for cirrhosis-rela–ted complications: an international position statement. JHEP Rep. 2023;5(8):100785. doi: 10.1016/j.jhepr.2023.100785.
- Mousa N, Elmetwalli A, Abdelsalam M, Wahba M, Selim M, Nour D, et al. Risk stratification of spontaneous bacterial peritonitis recurrence: integrating acute kidney injury, biomarkers, composite scores, and machine learning models. Gut Pathog. 2025;17(1):103. doi: 10.1186/s13099-025-00774-5.
- Tutchenko M, Rudyk D, Besedinskyi M, Chub S. Spontaneous bacterial peritonitis. East Ukr Med J. 2024;12(2):221-228. doi: 10.21272/eumj.2024;12(2):221-228.
- Nadim MK, Kellum JA, Forni L, Francoz C, Asrani SK, Ostermann M, et al. Acute kidney injury in patients with cirrhosis: Acute Disease Quality Initiative (ADQI) and International Club of Ascites (ICA) joint multidisciplinary consensus meeting. J Hepatol. 2024;81(1):163-183. doi: 10.1016/j.jhep.2024.03.031.
- Khan S, Linganna M. Diagnosis and management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome. Cleve Clin J Med. 2023;90(4):209-213. doi: 10.3949/ccjm.90a.22028.
- Kolosovych IV, Hanol IV, Cherepenko IV, Lebedieva KO, Korolova KO. Intraabdominal pressure and its correction in acute surgical pathology. Wiad Lek. 2022;75(2):372-376. doi: 10.36740/WLek202202108.
- Mutlu U, Genc Ulucecen S, Iliaz R, Atasoy A, Cavus B, Ciftcibasi Ormeci A, et al. Intra-abdominal hypertension and its prognostic impact on mortality in cirrhotic patients with ascites: the role of paracentesis. Turk J Gastroenterol. 2025;36(6):390-397. doi: 10.5152/tjg.2025.24375.
- Pereira RA, Virella D, Perdigoto R, Marcelino P, Saliba F, Germano N. Continuous passive paracentesis versus large-volume paracentesis in the prevention and treatment of intra-abdominal hypertension in the critically ill cirrhotic patient with ascites –(COPPTRIAHL): study protocol for a randomized controlled trial. Trials. 2023;24(1):534. doi: 10.1186/s13063-023-07541-4.
- Huang CH, Lee CH, Chang C. Spontaneous bacterial peritonitis in decompensated liver cirrhosis: a literature review. Livers. 2022;2(3):214-232. doi: 10.3390/livers2030018.
- Albillos A, Lario M, Álvarez-Mon M. Cirrhosis-associa–ted immune dysfunction: distinctive features and clinical relevance. J Hepatol. 2014;61(6):1385-1396. doi: 10.1016/j.jhep.2014.08.010.
- Zhang Y, Zhang J, Korff S, Ayoob F, Vodovotz Y, Billiar TR. Delayed neutralization of IL-6 reduces organ injury, selectively suppresses inflammatory mediator and partially normalizes immune dysfunction following trauma and hemorrhagic shock. Shock. 2014;42(3):218-227. doi: 10.1097/SHK.0000000000000211.
- Lupu D, Scârneciu CC, Țînț D, Tudoran C. Cirrhotic cardiomyopathy: bridging hepatic and cardiac pathophysiology in the modern era. J Clin Med. 2025;14(17):5993. doi: 10.3390/jcm14175993.
- Simbrunner B, Trauner M, Reiberger T, Mandorfer M. Recent advances in the understanding and management of hepatorenal syndrome. Fac Rev. 2021;10:48. doi: 10.12703/r/10-48.
- Badura K, Frąk W, Hajdys J, Majchrowicz G, Młynarska E, Rysz J, et al. Hepatorenal syndrome-novel insights into diagnostics and treatment. Int J Mol Sci. 2023;24(24):17469. doi: 10.3390/ijms242417469.
- Chen JW, Chen PF, Li J, Duan XH, Ren JZ, Zhang WG. Transjugular intrahepatic portosystemic shunt for preventing rebleeding of esophageal varices in patients with portal cavernous transformation. Dig Dis Sci. 2025;70(5):1897-1905. doi: 10.1007/s10620-025-08955-7.
- Kolosovych IV, Uzun H. Treatment tactics for gastric erosive-ulcerative bleeding on the background of liver cirrhosis. General Surgery. 2023;(3-4):46-51. doi: 10.30978/GS-2023-3-46.
- Lesmana CRA, Shukla A, Kumar A, Shalimar, Qi X, Gani RA, et al. Management of acute variceal bleeding: updated APASL guidelines. Hepatol Int. 2025;19(5):1003-1031. doi: 10.1007/s12072-025-10894-4.
- Yordanov A. Management algorithm in variceal upper gastrointestinal bleeding. Scripta Sci Med. 2026;58(1):38-48. doi: 10.14748/v1w7k930.
- Kola G, Sureshkumar S, Mohsina S, Sreenath GS, Kate V. Restrictive versus liberal transfusion strategy in upper gastrointestinal bleeding: a randomized controlled trial. Saudi J Gastroenterol. 2021;27(1):13-19. doi: 10.4103/sjg.SJG_152_20.
- Narayanan V, Devadas K, Sreesh S, Varghese J, Solanki R, Mohapatra SD, et al. Novel predictors of response to therapy with terlipressin and albumin in hepatorenal syndrome-acute kidney injury. Ann Gastroenterol. 2024;37(1):81-88. doi: 10.20524/aog.2023.0853.
- Rockey DC, Gordon F, Thuluvath PJ, Victor D, Kemmer N, Cardoza S, et al. Terlipressin for hepatorenal syndrome in patients with early-stage acute-on-chronic liver failure. Liver Int. 2025;45(12):e70399. doi: 10.1111/liv.70399.
- Shastri A, Rose S, Vojjala N, Bhagat N, De A. The “dark” side of terlipressin: a case report of ischemic skin necrosis and review of literature. Egypt Liver J. 2023;13:1-5. doi: 10.1186/s43066-023-00273-9.
- Ahmed AI, Kaleem MZ, Abbarh S, Barjas HH, Ismail A, Albuni MK, et al. Terlipressin-induced skin necrosis in cirrhotic patients: a case report and comprehensive literature review. Clin Case Rep. 2024;12(10):e9141. doi: 10.1002/ccr3.9141.