
Журнал «Травма» Том 27, №3, 2026
Вернуться к номеру
Біомеханічне обґрунтування технології позавогнищевого остеосинтезу при дефектах великогомілкової кістки під впливом стискаючого навантаження
Авторы: Бур’янов О.А. (1), Кваша В.П. (1), Ярмолюк Ю.О. (1, 2), Пасенко М.С. (1), Карпінський М.Ю. (3), Яресько О.В. (3)
(1) - Національний медичний університет імені О.О. Богомольця, м. Київ, Україна
(2) - Національний військово-медичний клінічний центр «Головний військовий клінічний госпіталь», м. Київ, Україна
(3) - ДУ «Інститут патології хребта та суглобів імені професора М.І. Ситенка НАМН України», м. Харків, Україна
Рубрики: Травматология и ортопедия
Разделы: Клинические исследования
Версия для печати
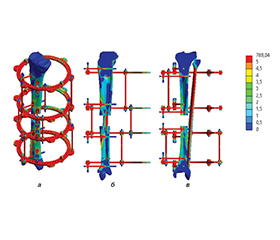
Актуальність. Довгі сегментарні дефекти великогомілкової кістки можуть виникнути внаслідок високоенергетичної травми, радикального видалення забруднених кісткових фрагментів при відкритому переломі, резекції пухлини кістки або при обробці інфікованих ділянок у місці незрощення. Повномасштабні бойові дії суттєво вплинули на статистичні показники дефектів великогомілкової кістки. Вогнепальні та мінно-вибухові ураження, які характеризуються високою кінетичною енергією, призвели до зростання частки первинних дефектів кісткової тканини довгих кісток нижніх кінцівок (за попередніми даними, близько 11–17 %). Одними з сучасних способів відновлення дефектів кісткової тканини є методика дистракційного остеогенезу, або кісткового транспорту, та методика Masquelet, кожна з яких має свої недоліки та переваги. Мета: дослідити напружено-деформований стан моделі гомілки з дефектом великогомілкової кістки в середній третині при різних варіантах її позавогнищевого остеосинтезу під впливом стискаючого навантаження. Матеріали та методи. У середній третині великогомілкової кістки моделювали дефект довжиною 5 см. Вивчали стабілізацію великогомілкової кістки апаратом зовнішньої фіксації (АЗФ) при трьох варіантах проведення стрижнів діаметром 8 мм під кутами 30°, 60° і 90°. Як скінченний елемент був обраний 10-вузловий тетраедр з квадратичною апроксимацією. Усім матеріалам, з яких складалися моделі, задавали відповідні механічні властивості, такі як модуль пружності Юнга та коефіцієнт Пуассона. Результати. Рівень напружень сягає максимуму навколо стрижнів 5 і 3 — 48,0 та 40,6 МПа відповідно. Навколо фронтальних гвинтів 1 і 7 відповідно в проксимальній та дистальній парах рівень напружень значно нижчий — 29,8 та 31,9 МПа. Максимальний рівень напружень визначений на стрижнях у парах, найближчих до зони дефекту, а саме в парі стрижнів 3 і 4 — 320,9 і 272,2 МПа відповідно, а також в парі стрижнів 5 і 6 — 276,6 та 256,6 МПа відповідно. Високий рівень напружень на стрижнях, розташованих поблизу зони дефекту, передається і на кільця АЗФ, до яких ці стрижні кріпляться. Так, найвищий рівень напружень —243,4 МПа — визначено в нижньо-середньому кільці, 239,6 МПа — у верхньо-середньому. У верхньому та нижньому кільцях напруження в 1,5–2 рази нижчі та визначаються на позначках 166,8 та 127,7 МПа відповідно. На стрижнях, які з’єднують кільця АЗФ між собою, картина протилежна. На середніх стрижнях визначено мінімальний рівень напружень — 152,3 МПа, а максимальної позначки 340,5 МПа напруження сягають у стрижнях верхньої секції. Напруження у стрижнях нижньої секції 170,9 МПа удвічі нижчі за верхні, але трохи вищі за напруження у стрижнях середньої секції. Висновки. За умов вертикального стискаючого навантаження найбільш сприятливим щодо мінімізації напружень у кістковій тканині є варіант монтажу АЗФ із проведенням фіксуючих стрижнів під кутом 30°. Зі збільшенням кута між стрижнями до 60° і 90° відзначається зменшення напружень у кільцях АЗФ, однак це не компенсує підвищення напружень у кістковій тканині та фіксуючих елементах. Максимальні значення напружень у всіх елементах АЗФ залишаються суттєво нижчими за межу міцності хірургічної сталі, що свідчить про достатній запас міцності конструкції.
Background. Long segmental defects of the tibia can occur as a result of high-energy trauma, radical removal of contaminated bone fragments in an open fracture, resection of a bone tumor, or during treatment of infected areas at the site of nonunion. Full-scale combat operations significantly affected the statistical indicators of tibial defects. Gunshot and mine-explosive injuries, which are characterized by high kinetic energy, have led to an increase in the proportion of primary defects in the long bones of the lower extremities (according to preliminary data, about 11–17 %). Among methods currently used for repairing bone tissue defects, there are the distraction osteogenesis technique, or bone transport, and the Masquelet technique, each of which has its own disadvantages and advantages. Objective of the study: to investigate the stress-strain state of a tibial model with a defect in its middle third, with different options for extra-articular osteosynthesis under the influence of compressive loading. Materials and methods. A defect of 5 cm long was modeled in the middle third of the tibia. Stabilization of the tibia with an external fixation device (EFD) was studied with three options for inserting rods with a diameter of 8 mm at angles of 30, 60, and 90°. A 10-node tetrahedron with quadratic approximation was chosen as the finite element. All materials used in the models were assigned appropriate mechanical properties, such as Young’s modulus and Poisson’s ratio. Results. The stress level reaches a maximum around rods 5 and 3 — 48.0 and 40.6 MPa, respectively. Around frontal screws 1 and 7, in the proximal and distal pairs, respectively, the stress level is significantly lower — 29.8 and 31.9 MPa. The maximum stress level is determined on the rods in the pairs closest to the defect zone, namely in the pair 3 and 4 (320.9 and 272.2 MPa, respectively), 5 and 6 (276.6 and 256.6 MPa). The high stress level on the rods located near the defect zone is also transmitted to the EFD rings to which these rods are attached. Thus, the highest stress level of 243.4 MPa was determined in the lower-middle ring and 239.6 MPa — in the upper-middle one. In the upper and lower rings, stresses are 1.5–2 times lower and are determined at 166.8 and 127.7 MPa, respectively. On the rods that connect the EFD rings to each other, the picture is the opposite. The minimum stress level was determined on the middle rods — 152.3 MPa, the maximum stress level of 340.5 MPa is reached in the rods of the upper section. The stress in the rods of the lower section is 170.9 MPa, half the upper ones, but slightly higher than in the rods of the middle section. Conclusions. Under conditions of vertical compressive load, the most favorable option for minimizing stresses in bone tissue is the use of an EFD with insertion of the fixing rods at an angle of 30°. With an increase in the angle between the rods to 60 and 90°, there is a decrease in stresses in the EFD rings; however, this does not compensate for an increase in stresses in the bone tissue and fixing elements. The maximum stress values in all elements of an EFD remain significantly lower than the tensile strength of surgical steel, which indicates a sufficient safety margin of the structure.
кістковий дефект; кістковий транспорт; позавогнищевий остеосинтез; напружено-деформований стан моделі
bone defect; bone transport; extra-articular osteosynthesis; stress-strain state of the model