
Журнал «Травма» Том 27, №3, 2026
Вернуться к номеру
Хірургічне лікування вивиху головки стегнової кістки в дітей із ДЦП: мультицентровий ретроспективний аналіз серії зі 171 пацієнта (повідомлення перше)
Авторы: D.V. Yershov (1), O.I. Korolkov (2), F.V. Klymovytskyi (1), A.V. Chornenkyi (3), P.M. Rakhman (4)
(1) - Donetsk National Medical University, Lyman — Kropyvnytskyi, Ukraine
(2) - Clinical Center of Children’s Healthcare (Lviv Regional Children’s Clinical Hospital “Okhmatdyt”), Lviv, Ukraine
(3) - Dnipro City Multidisciplinary Clinical Hospital for Mothers and Children named after prof. M.F. Rudnev (Rudnev Mother and Child Center), Dnipro, Ukraine
(4) - Medical Center “MedGarden”, Chernivtsi, Ukraine
Рубрики: Травматология и ортопедия
Разделы: Клинические исследования
Версия для печати
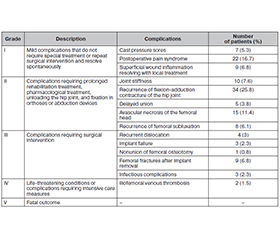
Актуальність. Вивих голівки стегнової кістки (ВГСК) залишається серйозним ортопедичним ускладненням у дітей iз діагнозом ДЦП, яке призводить до обмеження рухів у кульшовому суглобі, больового синдрому та прогресуючих порушень якості життя пацієнтів. Мета: оцінити рентгенологічні й клінічні результати, а також частоту ускладнень після реконструктивної операції з приводу ВГСК у дітей із ДЦП (рівні GMFCS III–V). Матеріали та методи. Критерії включення в дослідження: ВГСК (індекс міграції ≥ 100 %) у дітей віком від 4 до 18 років із діагнозом ДЦП, GMFCS III–V рівнів, яким виконано хірургічно відкрите вправлення та реконструкцію кульшового суглоба. У досліджувану групу увійшов 171 пацієнт (226 суглобів). Проведено аналіз коморбідності, оцінку клінічних симптомів, рентгенологічних параметрів кульшових суглобів до та після хірургічного лікування, а також ускладнень за модифікованою класифікацією Clavien — Dindo. Середній вік пацієнтів становив 8 років 8 міс. Середній термін спостереження в післяопераційному періоді дорівнював 3,0 року ± 6,5 міс. У 37 пацієнтів (21 %) відзначався високий вивих стегна. Результати. Проведене хірургічне лікування дозволило статистично значущо змінити рентгенологічні показники, як-от індекс міграції, кут Віберга, ацетабулярний індекс, шийково-діафізарний кут, та клінічні симптоми: зменшити біль в ділянці кульшового суглоба, поліпшити рухи в ньому. При цьому зафіксовано значну частоту ускладнень (n = 132, 226 стегон), серед яких 16,6 % випадків потребували проведення додаткових хірургічних втручань (рівень III–IV за класифікацією Clavien — Dindo). Найпоширенішими ускладненнями були рецидив контрактури, аваскулярний некроз та переломи стегнової кістки після видалення імплантату. Висновки. Хірургічне лікування ВГСК у дітей із ДЦП (GMFCS III–V) приводить до вірогідного поліпшення клініко-рентгенологічних показників, однак супроводжується відносно великою кількістю ускладнень. Ці результати підкреслюють важливість раннього впровадження програм спостереження та ретельного відбору пацієнтів.
Background. Hip dislocation remains a serious orthopedic complication in children with cerebral palsy (CP), leading to restricted hip joint mobility, pain syndrome, and progressive decline in the patients’ quality of life. Aim: to evaluate radiographic and clinical outcomes, as well as complication rates, following reconstructive surgery for hip dislocation in children with CP (GMFCS levels III–V). Materials and methods. Inclusion criteria: children with CP aged 4 to 18 years with hip dislocation (migration index ≥ 100 %), and GMFCS levels III–V, who underwent open reduction and hip joint reconstruction. The study group included 171 patients (226 joints). The analysis covered comorbidity, clinical symptoms, and radiographic parameters of the hip joints before and after surgery, as well as complications according to the modified Clavien-Dindo scale. The mean age of patients was 8 years and 8 months. The mean postoperative follow-up period was 3.0 years ± 6.5 months. High hip dislocation was observed in 37 patients (21.6 %). Results. Surgical reconstruction resulted in significant improvement in radiographic parameters, including reduction of migration index and acetabular index, and correction of femoral alignment. Clinical improvement was observed in pain reduction and range of motion. However, a high complication rate was recorded (132 complications in 226 hips), with 16.6 % requiring additional surgical intervention (Clavien-Dindo grade III–IV). The most common complications included recurrent contracture, avascular necrosis, and femoral fractures after implant removal. Conclusions. Reconstructive hip surgery for hip dislocation in children with CP (GMFCS III–V) results in significant improvement in radiographic parameters and clinical outcomes but is associated with a substantial complication rate. These findings highlight the importance of early surveillance programs and careful patient selection.
вивих стегна; дитячий церебральний параліч; хірургічне лікування; остеотомія таза; остеотомія стегнової кістки; хірургічні ускладнення
hip dislocation; cerebral palsy; surgical treatment; pelvic osteotomy; femoral osteotomy; surgical complications