
Международный эндокринологический журнал Том 16, №6, 2020
Вернуться к номеру
Can metastasis and recurrence be detected with Endocan and Vascular Endothelial Growth Factor in thyroid papillary cancer?
Авторы: Hande Peynirci(1), Canan Ersoy(2), Pınar Sisman(3), Ozlem Saraydaroglu(4), Coskun Ozer Demirtas(5), Ozen Oz Gul(2)
(1) — Health Sciences University Kanuni Sultan Suleyman Training and Research Hospital, Department of Endocrinology and Metabolism Diseases, Istanbul, Turkey
(2) — Uludag University Faculty of Medicine, Department of Internal Medicine, Division of Endocrinology and Metabolism Diseases, Bursa, Turkey
(3) — Private Medicana Hospital, Department of Endocrinology and Metabolism Diseases, Bursa, Turkey
(4) — Uludag University Faculty of Medicine, Department of Pathology, Bursa, Turkey
(5) — Marmara University Faculty of Medicine, Department of Internal Medicine, Division of Gastroenterology, Istanbul, Turkey
Рубрики: Эндокринология
Разделы: Клинические исследования
Версия для печати
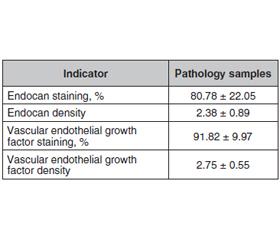
Актуальність. Відомо, що ендокан асоціюється з різними типами злоякісних утворень. Установлено, що фактор росту судинного ендотелію (VEGF) підвищує експресію ендокану. Метою проведеного дослідження було виявлення наявності рецидиву захворювання та/або метастазування за допомогою змін ендокану та VEGF у пацієнтів із папілярним раком щитоподібної залози. Матеріали та методи. Ретроспективне дослідження проводилося від січня 2005 року до грудня 2015 року. Реєстрували стать, вік, а також вік пацієнта на час діагностики тиреоїдного раку, тривалість спостереження. Дослідну групу було розподілено на дві групи, які становили пацієнти з післяопераційними рецидивами і/або метастазами та без них. Патологічні зразки обробляли Anti-ESM-1 та Anti-VEGFA, оцінювали відсоток забарвлення та щільність. Результати. Під спостереженням перебували 59 пацієнтів (43 жінки та 16 чоловіків). Середній вік становив 52,39 ± 13,75 року. Установлено, що в середньому найдовший діаметр пухлини становив 21,31 ± 20,20 мм, а тривалість спостереження — 37,24 ± 32,68 місяця. Серед пацієнтів 54,2 % мали рецидив та/або метастазування, тоді як у 45,8 % рецидиву чи метастазування не спостерігалося. Відсоток щільності ендокану становив 84,26 ± 20,32 та 2,56 ± 0,75 у групі рецидивів та/або метастазів, 75,56 ± 24,06 та 2,11 ± 1,02 — відповідно у групі без них. Щільність ендокану була вищою в пацієнтів із рецидивом та/або метастазами, але не досягла статистичної значущості (р = 0,077, р = 0,136 відповідно). Істотної різниці між двома групами щодо забарвлення та щільності VEGF не виявлено. Висновки. Необхідні подальші дослідження для оцінки ролі ендокану та фактора росту судинного ендотелію для прогнозування рецидиву та/або метастазування папілярної карциноми щитоподібної залози.
Актуальность. Известно, что эндокан ассоциируется с различными типами злокачественных образований. Установлено, что фактор роста сосудистого эндотелия (VEGF) повышает экспрессию эндокана. Целью проведенного исследования было выявление наличия рецидива заболевания и/или метастазирования с помощью изменений эндокана и VEGF у пациентов с папиллярным раком щитовидной железы. Материалы и методы. Ретроспективное исследование проводилось с января 2005 года по декабрь 2015 года. Регистрировали пол, возраст, а также возраст пациента на момент диагностики тиреоидного рака, продолжительность наблюдения. Исследовательская группа была разделена на две подгруппы, которые составили пациенты с послеоперационными рецидивами и/или метастазами и без них. Патологические образцы обрабатывали Anti-ESM-1 и Anti-VEGFA, оценивали процент окрашивания и плотность. Результаты. Под наблюдением находились 59 пациентов (43 женщины и 16 мужчин). Средний возраст составил 52,39 ± 13,75 года. Установлено, что наиболее длинный диаметр опухоли составил 21,31 ± 20,20 мм, а продолжительность наблюдения — 37,24 ± 32,68 месяца. Среди пациентов 54,2 % имели рецидив и/или метастазирование, тогда как у 45,8 % рецидива или метастазирования не наблюдалось. Процент плотности эндокана составил 84,26 ± 20,32 и 2,56 ± 0,75 в группе рецидивов и/или метастазов, 75,56 ± 24,06 и 2,11 ± 1,02 — соответственно в группе без них. Плотность эндокана была выше у пациентов с рецидивом и/или метастазами, но не достигла статистической значимости (р = 0,077, р = 0,136 соответственно). Существенной разницы между двумя группами по окраске и плотности VEGF не обнаружено. Выводы. Необходимы дальнейшие исследования для оценки роли эндокана и фактора роста сосудистого эндотелия для прогнозирования рецидива и/или метастазирования папиллярной карциномы щитовидной железы.
Background. Endocan is known to be associated with different type of malignancies and vascular endothelial growth factor (VEGF) has been shown to upregulate endocan expression. We purposed to determine whether the presence of disease recurrence and/or metastasis can be detected with pathological evaluation of endocan and VEGF in patients with thyroid papillary cancer. Materials and methods. This study was performed retrospectively between January 2005 and December 2015. Patients’ gender, age, also age at diagnosis, and duration of follow-up were recorded. The study group was divided into two groups comprised of patients with and without postoperative recurrence and/or metastasis. Pathological samples were treated with Anti-ESM-1 and Anti-VEGFA, staining percentage and density were evaluated. Results. A total of 59 patients (43 female and 16 male) were included. The mean age was 52.39 ± 13.75 years. Mean longest tumor diameter was found to be 21.31 ± 20.20 mm, and follow-up duration was 37.24 ± 32.68 months. Among the patients, 54.2 % had recurrence and/or metastasis, while 45.8 % did not have either. The percentage of endocan staining and density was 84.26 ± 20.32 and 2.56 ± 0.75 in the recurrence and/or metastases group, 75.56 ± 24.06 and 2.11 ± 1.02, respectively in the group without. Endocan staining and density was higher in the patients with recurrence and/or metastasis but not statistically significant (p = 0.077, p = 0.136, respectively). No significant difference was found between two groups in terms of VEGF staining and density. Conclusions. These markers might be further evaluated for determination their role in recurrence and/or metastasis of thyroid papillary carcinoma.
папілярний рак щитоподібної залози; ендокан; фактор росту судинного ендотелію; рецидив; метастазування
папиллярный рак щитовидной железы; эндокан; фактор роста сосудистого эндотелия; рецидив; метастазирование
thyroid papillary cancer; endocan; vascular endothelial growth factor; recurrence; metastasis
Introduction
Materials and methods
Results
/75.jpg)
/76.jpg)
Discussion
Conclusions
Additional information
- Davies L., Welch H.G. Current thyroid trends in the United States. JAMA Otolaryngol Head Neck Surg. 2014. 140(4). 317-322. doi: 10.1001/jamaoto.2014.1.
- Eustatia-Rutten C.F., Corssmit E.P., Biermasz N.R., Pereira A.M., Romijn J.A., Smit J.W. Survival and death causes in differentiated thyroid carcinoma. J. Clin. Endocrinol. Metab. 2006. 91(1). 313-319. doi: 10.1210/jc.2005-1322.
- Kali A., Shetty K.S. Endocan: a novel circulating proteoglycan. Indian J. Pharmacol. 2014. 46(6). 579-583. doi: 10.4103/0253-7613.144891.
- Balta S., Mikhailidis D.P., Demirkol S., Ozturk C., Celik T., Iyisoy A. Endocan: A novel inflammatory indicator in cardiovascular disease? Atherosclerosis. 2015. 243(1). 339-343. doi: 10.1016/ j.atherosclerosis. 2015.09.030.
- Sarrazin S., Adam E., Lyon M. et al. Endocan or endothelial cell specific molecule-1 (ESM-1): a potential novel endothelial cell marker and a new target for cancer therapy. Biochim. Biophys. Acta. 2006. 1765(1). 25-37. doi: 10.1016/j.bbcan.2005.08.004.
- Ferrara N. Vascular endothelial growth factor: basic science and clinical progress. Endocr. Rev. 2004. 25(4). 581-611. doi: 10.1210/er.2003-0027.
- Soh E.Y., Duh Q.Y., Sobhi S.A. et al. Vascular endothelial growth factor expression is higher in differentiated thyroid cancer than in normal or benign thyroid. J. Clin. Endocrinol. Metab. 1997. 82(11). 3741-3747. doi: 10.1210/jcem.82.11.4340.
- Rennel E., Mellberg S., Dimberg A. et al. Endocan is a VEGF-A and PI3K regulated gene with increased expression in human renal cancer. Exp. Cell. Res. 2007. 313(7). 1285-1294. doi: 10.1016/j.yexcr.2007.01.021.
- Delehedde M., Devenyns L., Maurage C.A., Vivès R.R. Endocan in Cancers: A Lesson from a Circulating Dermatan Sulfate Proteoglycan. Int. J. Cell. Biol. 2013. 2013. 705027. doi: 10.1155/2013/705027.
- Yang J., Yang Q., Yu S., Zhang X. Endocan: A new marker for cancer and a target for cancer therapy. Biomed. Rep. 2015. 3(3). 279-283. doi: 10.3892/br.2015.438.
- Mazzaferri E.L., Jhiang S.M. Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Am. J. Med. 1994. 97(5). 418-428. doi: 10.1016/0002-9343(94)90321-2.
- Soares P., Celestino R., Melo M., Fonseca E., Sobrinho-Simões M. Prognostic biomarkers in thyroid cancer. Virchows Arch. 2014. 464(4). 333-346. doi: 10.1007/s00428-013-1521-2.
- Shi Y., Su C., Hu H. et al. Serum MMP-2 as a potential predictive marker for papillary thyroid carcinoma. PLoS One. 2018. 13(6). e0198896. doi: 10.1371/journal.pone.0198896.
- Zarkesh M., Zadeh-Vakili A., Akbarzadeh M., Fanaei S.A., Hedayati M., Azizi F. The role of matrix metalloproteinase-9 as a prognostic biomarker in papillary thyroid cancer. BMC Cancer. 2018. 18(1). 1199. doi: 10.1186/s12885-018-5112-0.
- Lassalle P., Molet S., Janin A. et al. ESM-1 is a novel human endothelial cell-specific molecule expressed in lung and regulated by cytokines. J. Biol. Chem. 1996. 271(34). 20458-20464. doi: 10.1074/jbc.271.34.20458.
- Tı́már J., Lapis K., Dudás J., Sebestyén A., Kopper L., Kovalszky I. Proteoglycans and tumor progression: Janus-faced molecules with contradictory functions in cancer. Semin. Cancer Biol. 2002. 12(3). 173-186. doi: 10.1016/S1044-579X(02)00021-4.
- Delehedde M., Lortat-Jacob H., Gallagher J.T. et al. Proteoglycan involvement in inflammatory diseases. new developments in GAG-based therapies. Medicinal Chemistry Reviews-Online. 2005. 2. 345-357. doi: 10.2174/1567203054637560.
- Scherpereel A., Gentina T., Grigoriu B. et al. Overexpression of endocan induces tumor formation. Cancer Res. 2003. 63(18). 6084-6089.
- Chen L.Y., Liu X., Wang S.L., Qin C.Y. Over-expression of the Endocan gene in endothelial cells from hepatocellular carcinoma is associated with angiogenesis and tumour invasion. J. Int. Med. Res. 2010. 38(2). 498-510. doi: 10.1177/147323001003800213.
- Kang Y.H., Ji N.Y., Han S.R. et al. ESM-1 regulates cell growth and metastatic process through activation of NF-kappaB in colorectal cancer. Cell. Signal. 2012. 24(10). 1940-1949. doi: 10.1016/j.cellsig.2012.06.004.
- Liu N., Zhang L.H., Du H. et al. Overexpression of endothelial cell specific molecule-1 (ESM-1) in gastric cancer. Ann. Surg. Oncol. 2010. 17(10). 2628-2639. doi: 10.1245/s10434-010-1037-9.
- Béchard D., Scherpereel A., Hammad H. et al. Human endothelial-cell specific molecule-1 binds directly to the integrin CD11a/CD18 (LFA-1) and blocks binding to intercellular adhesion molecule-1. J. Immunol. 2001. 167(6). 3099-3106. doi: 10.4049/jimmunol.167.6.3099.
- Arpaci D., Karakece E., Tocoğlu A.G. et al. Endocan, TGF-beta, and ADMA as risk factors for endothelial dysfunction and possible vascular disease in patients with subclinical hypothyroidism. Ann. Clin. Lab. Sci. 2016. 46(6). 601-607.
- Shibuya M., Claesson-Welsh L. Signal transduction by VEGF receptors in regulation of angiogenesis and lymphangiogenesis. Exp. Cell. Res. 2006. 312(5). 549-560. doi: 10.1016/j.yexcr.2005.11.012.
- Klein M., Vignaud J.M., Hennequin V. et al. Increased expression of the vascular endothelial growth factor is a pejorative prognosis marker in papillary thyroid carcinoma. J. Clin. Endocrinol. Metab. 2001. 86(2). 656-658. doi: 10.1016/j.yexcr.2005.11.012.
- Ferrara N., Davis-Smyth T. The biology of vascular endothelial growth factor. Endocr. Rev. 1997. 18(1). 4-25. doi: 10.1210/edrv.18.1.0287.
- Lennard C.M., Patel A., Wilson J. et al. Intensity of vascular endothelial growth factor expression is associated with increased risk of recurrence and decreased disease-free survival in papillary thyroid cancer. Surgery. 2001. 129(5). 552-558. doi: 10.1067/msy.2001.112592.
- Kilicarslan A.B., Ogus M., Arici C., Pestereli H.E., Cakir M., Karpuzoglu G. Clinical importance of vascular endothelial growth factor (VEGF) for papillary thyroid carcinomas APMIS. 2003. 111(3). 439-443. doi: 10.1034/j.1600-0463.2003.t01-1-1110209.x.
- Karaca Z., Tanriverdi F., Unluhizarci K. et al. VEGFR1 expression is related to lymph node metastasis and serum VEGF may be a marker of progression in the follow-up of patients with differentiated thyroid carcinoma. Eur. J. Endocrinol. 2011. 164(2). 277-284. doi: 10.1530/EJE-10-0967.
- Mohamad Pakarul Razy N.H., Wan Abdul Rahman W.F., Win T.T. Expression of Vascular Endothelial Growth Factor and Its Receptors in Thyroid Nodular Hyperplasia and Papillary Thyroid Carcinoma: A Tertiary Health Care Centre Based Study. Asian Pac. J. Cancer Prev. 2019. 20(1). 277-282. doi: 10.31557/APJCP.2019.20.1.277.