
Архив офтальмологии Украины Том 12, №1, 2024
Вернуться к номеру
Оцінка ризику прогресування діабетичної ретинопатії у хворих на цукровий діабет 2-го типу на тлі гіповітамінозу D
Авторы: Риков С.О., Нетребін Л.І.
Інститут післядипломної освіти, Національний медичний університет імені О.О. Богомольця, м. Київ, Україна
Рубрики: Офтальмология
Разделы: Клинические исследования
Версия для печати
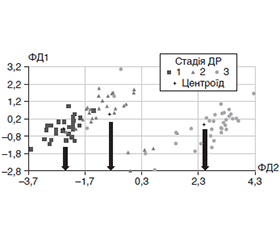
Актуальність. Діабетична ретинопатія (ДР) є одним із найсерйозніших ускладнень діабету, що вражає майже 40 % хворих на ЦД, є однією з головних причин сліпоти серед людей віком до 50 років із показником 4,8 %. Контроль компенсації ЦД є ключовим компонентом запобігання ДР, але не єдиним. Показано, що гіповітаміноз D бере участь у патогенезі ЦД 2-го типу та може відігравати негативну роль у формуванні та перебігу ДР. Методи оцінки ризику прогресування ДР у хворих на ЦД 2-го типу на тлі дефіциту вітаміну D в літературі поодинокі. Мета роботи полягала у розробці математичної моделі оцінки ризику прогресування ДР у хворих на ЦД 2-го типу на тлі гіповітамінозу D із використанням дискримінантного аналізу. Матеріали та методи. Проведено одноцентрове одномоментне відкрите вибіркове спостережне дослідження у хворих на ДР за ЦД 2-го типу. Включення пацієнтів у групи з ДР відбувалося відповідно до протоколу ETDRS (2019) та Наказу МОЗ України від 22.05.2009 № 356 в редакції Наказу МОЗ України від 05.08.2009 № 574. Головними критеріями невключення були ЦД 1-го типу, хвороби та стани, що супроводжуються порушенням фосфорно-кальцієвого обміну, а також пошкодження зорового нерва, клінічно значуща макулопатія, глаукома, зріла катаракта. Дослідження проведено у 90 пацієнтів (173 ока) з ДР (чоловіки та жінки, середній вік 59,4 ± 3,6 (± SD) року, середній рівень глікованого гемоглобіну 7,88 ± 0,62 (± SD) %), яких залежно від стадії ДР розділили на 3 групи. У групу контролю були включені практично здорові без ЦД в анамнезі відповідно до критеріїв невключення (62 людини, середній вік 51,5 ± 13,3 (± SD) року). Концентрацію HbA1c у крові визначали методом високошвидкісної колонкової рідинної хроматографії, 25(OH)D — хемілюмінесцентним імунним аналізом. Статистичний аналіз включав дисперсійний і дискримінантний аналіз. Результати. Оцінка ризику прогресування ДР у хворих на ЦД 2-го типу на тлі дефіциту 25(ОН)D включає кілька етапів. На 1-му етапі досліджують концентрацію в крові 25-гідроксивітаміну D та вміст HbA1с. Далі хворому надаються коди антидіабетичної терапії (ВидТер) (пероральний цукрознижувальний препарат — 0, інсулінотерапія — 1), статі (жінки — 2, чоловіки — 1) та визначається вік. На 2-му етапі підраховуються функції класифікації — ФК1, ФК2 та ФК3 і за результатами обчислення ФК приймається рішення щодо приналежності до тієї групи, що відповідає найбільшому численному значенню одної з трьох ФК. На 3-му етапі порівнюють ФК1 з ФК2 або ФК2 з ФК3. Прогностичне рішення приймається як вибір тієї ФК, яка має більше значення. Так, якщо ФК1 > ФК2, то прогноз позитивний (стабілізація процесу на І або ІІ стадії). Якщо ФК2 > ФК3, то прогноз також відносно позитивний (стабілізація процесу на ІІ стадії). Якщо ФК1 < ФК2 або ФК2 < ФК3, то прогноз негативний, є ймовірність прогресування патологічного процесу до наступної стадії або навіть у межах ІІІ стадії. Висновки. Наведена модель оцінки ризику прогресування ДР у хворих на ЦД 2-го типу на тлі гіповітамінозу D має вірогідну інформативність у 88,89 % (Р < 0,0001).
Background. Diabetic retinopathy (DR) is one of the most serious complications of diabetes mellitus (DM), affecting almost 40 % of diabetic patients, and is one of the leading causes of blindness among people under 50 years of age with a rate of 4.8 %. Control of DM compensation is a key component of DR prevention, but not the only one. It has been shown that hypovitaminosis D is involved in the pathogenesis of type 2 DM and can play a negative role in the formation and course of DR. There are few methods in the literature for assessing the risk of DR progression in patients with type 2 DM against the background of vitamin D deficiency. The purpose of this work was to develop a mathematical model for assessing the risk of progression of DR in patients with type 2 DM on the background of hypovitaminosis D using discriminant analysis. Materials and methods. An open-label observational study was conducted among patients with type 2 DM and DR. However, our study has some limitations. The inclusion of patients in groups with DR was occurred in accordance with the ETDRS (2019) protocol and the Order of the Ministry of Health of Ukraine No. 356 dated May 22, 2009 as amended by the Order of the Ministry of Health of Ukraine No. 574 dated August 5, 2009. The main exclusion criteria were type 1 diabetes mellitus, diseases and conditions accompanied by impaired phosphorus-calcium metabolism, as well as damage to the optic nerve, clinically significant maculopathy, glaucoma, and mature cataract. This study was conducted in 90 patients (173 eyes) with DR (men and women with an average age of 59.4 ± 3.6 (± SD) years, average level of glycated hemoglobin of 7.88 ± 0.62 (± SD) %) who were divided into 3 groups depending on the stage of DR. The control group included practically healthy individuals without a history of diabetes mellitus according to the exclusion criteria (62 people with an average age of 51.5 ± 13.3 (± SD) years). The concentration of HbA1c in blood was determined by high-performance liquid chromatography, 25(OH)D by chemiluminescent immunoassay. Statistical analysis included variance and discriminant analysis. Results. Assessment of the risk of DR progression in patients with type 2 DM on the background of 25(OH)D deficiency includes several stages. At the stage I, the blood concentration of 25-hydroxyvitamin D and the content of HbA1c are examined. Next, the patient is given the codes of antidiabetic therapy (oral hypoglycemic drug — 0, insulin therapy — 1), gender (women — 2, men — 1) and age is determined. At the stage II, the functions of classification are calculated — FC1, FC2, FC3, and based on the results of this calculations, a decision is made regarding membership in the group that corresponds to the largest numerical value of one of the three FCs. At the stage III, FC1 is compared with FC2 or FC2 with FC3. The prognostic decision is taken as the choice of the FC that is more important. So, if FC1 > FC2, the prognosis is positive (stabilization of the process at the stage I or II). If FC2 > FC3, the prognosis is also relatively positive (stabilization of the process at the stage II). If FC1 < FC2 or FC2 < FC3, then the prognosis is negative, there is a possibility of progression of the pathological process to the next stage or even within the stage III. Conclusions. The presented model for assessing the risk of progression of DR in patients with type 2 DM against the background of hypovitaminosis D has a statistically significant informative value of 88.89 % (р < 0.0001).
діабетична ретинопатія; цукровий діабет 2-го типу; гіповітаміноз D
diabetic retinopathy; type 2 diabetes; hypovitaminosis D
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Sun H, Saeedi P, Karuranga S, et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022 Jan;183:109119. doi: 10.1016/j.diabres.2021.109119.
- Solomon SD, Goldberg MF. ETDRS Grading of Diabetic Re–tinopathy: Still the Gold Standard? Ophthalmic Res. 2019;62(4):190-195. https://doi.org/10.1159/000501372.
- Kyryliuk M, Іshchenko V. Pathogenesis of diabetic retino–pathy: a literature review. International Journal оf Endocrinology (Ukraine). 2019;15(7):567-575. https://doi.org/10.22141/2224-0721.15.7.2019.186061.
- Tecilazich F, Formenti AM, Giustina A. Role of vitamin D in diabetic retinopathy: Pathophysiological and clinical aspects. Rev Endocr Metab Disord. 2021 Dec;22(4):715-727. doi: 10.1007/s11154-020-09575-4.
- Maghbooli Z, Ebrahimi Meimand S, Malek Hosseini AA, et al. Alterations in circulating levels of vitamin D binding protein, total and bioavailability of vitamin D in diabetic retinopathy patients. BMC Endocr Disord. 2022 Jul 1;22(1):169. https://doi.org/10.1186/s12902-022-01084-6.
- Seyyar SA, Tokuc EO, Tıskaoğlu NS, et al. Do serum vitamin D levels correlate with Macular Edema or with Diabetic Retinopathy? Eur J Ophthalmol. 2022 Nov;32(6):3592-3598. https://doi.org/10.1177/11206721221076701.
- Ren Z, Li W, Zhao Q, Ma L, Zhu J. The impact of 1,25-dihydroxy vitamin D3 on the expressions of vascular endothelial growth factor and transforming growth factor–beta(1) in the retinas of rats with diabetes. Diabetes Res Clin. Pract. 2012;98:474-480. https://doi.org/10.1074/jbc.M112.386912.
- Cashman KD, Dowling KG, Škrabáková Z, et al. Vitamin D deficiency in Europe: pandemic? Am J Clin Nutr. 2016;103:1033-1044. doi: 10.3945/ajcn.115.120873.
- Комісаренко Ю.І. Вітамін D та його роль у регуляції метаболічних розладів при цукровому діабеті. Ліки України. 2013. 4. 51-54. http://nbuv.gov.ua/UJRN/likukr_2013_4_11.
- Pankiv VI, Yuzvenko TYu, Pashkovska NV, Pankiv IV. The relationship between serum vitamin D concentrations and development of diabetic retinopathy in type 2 diabetes mellitus. Mìžnarodnij endokrinologìčnij žurnal. 2022;18(8):432-435. doi: 10.22141/2224-0721.18.8.2022.1221.
- Netrebin L, Pankiv V, Kyryliuk M. Mathematical model for assessing the prognostic significance of 25(OH)D deficiency in the progression of diabetic retinopathy in type 2 diabetes patients. International Journal оf Endocrinology (Ukraine). 2023;19(4):269-273. https://doi.org/10.22141/2224-0721.19.4.2023.1284.
- Clemens TL, Henderson SL, Adams JS, Holick MF. Increased skin pigment reduces the capacity of skin to synthesise vitamin D3. Lancet. 1982;1:74-76. doi: 10.1016/s0140-6736(82)90214-8.