
Журнал «Почки» Том 13, №2, 2024
Вернуться к номеру
Досвід використання черезшкірної нефролітотомії в лікарні вторинної допомоги на Балі
Авторы: I Gede Yogi Prema Ananda, Herman Yudawan, I Gusti Lanang Andi Suharibawa
Klungkung General Hospital, Semarapura Kauh Klungkung, Bali, Indonesia
Рубрики: Нефрология
Разделы: Клинические исследования
Версия для печати
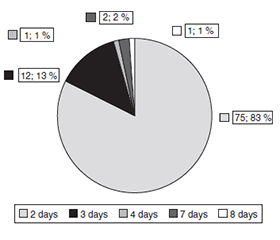
Актуальність. Утворення каменів у нирках є результатом накопичення кристалів. Черезшкірна нефролітотомія (ЧШНЛ) є кращим методом лікування при каменях розміром понад 2 см. Мета: проаналізувати результати й досвід використання ЧШНЛ при видаленні каменів у нирках. Матеріали та методи. Це було описове дослідження з перехресним дизайном, у якому використано вторинні дані з електронних медичних записів лікарні загального профілю (Клункунг, Індонезія). У період із жовтня 2020 року по серпень 2023 року за допомогою методу загальної вибірки проаналізовано 91 випадок. Аналіз проводився з використанням пакета SPSS Statistics 26. Результати. Найчастіше ЧШНЛ виконували у віковій групі 51–60 років (38,5 % пацієнтів). Найпоширенішим типом каменю був одиночний (48,4 %) із середнім розміром 3,570 ± 1,159 см. Середня тривалість процедури становила 38,630 ± 21,667 хв, одноразову пункцію застосовували в 68,1 % випадків. Рівень відчутого болю загалом був низьким, із середньою оцінкою 2 бали за 10-бальною шкалою. Середня тривалість перебування в лікарні становила 2,330 ± 1,012 дня. Результати ЧШНЛ у пацієнтів із сечокам’яною хворобою були сприятливими, з високим показником повного видалення каменів (92,3 %) і мінімальними ускладненнями. Післяопераційні ускладнення зустрічались нечасто. Висновки. Вважається, що ЧШНЛ є ефективною та безпечною процедурою при видаленні каменів у нирках.
Background. The formation of kidney stones is the result of the accumulation of crystals within the kidneys. Percutaneous nephrolithotomy (PCNL) is the preferred method for treating stones larger than 2 cm. This study aims to analyse outcomes and experiences of PCNL for kidney stone removal. Materials and methods. It was a descriptive study with a cross-sectional design, utilizing secondary data from electronic medical records in Klungkung General Hospital. There are 91 samples collected using total sampling between October 2020 and August 2023. The analysis was conducted using the SPSS Statistics 26. Results. The 51–60 age group (38.5 %) exhibited the highest prevalence of patients undergoing PCNL surgery. The most common type of stone was solitary (48.4 % of cases), with an average size of 3.570 ± 1.159 cm. The mean duration of the procedure was 38.630 ± 21.667 minutes, with a single puncture utilized in 68.1 % of cases. The pain levels experienced were generally low, with a mean score of 2 on a 10-point scale. The mean length of hospital stay was 2.330 ± 1.012 days. The outcomes of PCNL in patients with kidney stones were favourable, with a high stone-free rate of 92.3 % and minimal complications. Рostoperative complications were infrequent. Conclusions. It is suggested that PCNL is an effective and safe procedure for kidney stone removal.
черезшкірна нефролітотомія; нирковий камінь; вторинна лікарня; показник повного видалення каменів
percutaneous nephrolithotomy; kidney stone; secondary hospital; stone-free rate
Introduction
Materials and methods
Results
/40.jpg)
/40_2.jpg)
/41.jpg)
Discussion
Conclusions
- Alelign T, Petros B. Kidney Stone Disease: An Update on Current Concepts. Advances in Urology. 2018;2018.
- Mishra NK. Renal Calculi (Kidney Stones) and its Therapy. IGJPS. 2019;9(1):1-4. Available from: http://www.iglobaljournal.com/wp-content/uploads/2019/07/1.-Mishra-NK-2019.pdf.
- Edvardsson VO, Indridason OS, Haraldsson G, Kjartansson O, Palsson R. Temporal trends in the incidence of kidney stone disease. Clinical Investigation. 2013;83(1):146-52.
- Ferraro PM, Taylor EN, Curhan GC. Factors associated with sex differences in the risk of kidney stones. Nephrology Dialysis Transplantation. 2023 Jan 23;38(1):177-83. Available from: https://academic.oup.com/ndt/article/38/1/177/6524918.
- Sigurjonsdottir VK, Runolfsdottir HL, Indridason OS, Palsson R, Edvardsson VO. Impact of nephrolithiasis on kidney function. BMC Nephrology. 2015;16(1):1-7.
- Khalili P, Jamali Z, Sadeghi T, Esmaeili-nadimi A, Mohamadi M, Moghadam-Ahmadi A, et al. Risk factors of kidney stone disease: a cross-sectional study in the southeast of Iran. BMC Urology. 2021;21(1):1-8.
- NG118. Renal and ureteric stones: assessment and management. NICE. 2019;1-34.
- Ganpule AP, Vijayakumar M, Malpani A, Desai MR. Percutaneous nephrolithotomy (PCNL) a critical review. International Journal of Surgery. 2016;36(D):660-4.
- Karakeçi A, Karakoç O, Ozan T, Fırdolaş F, Tektaş C, Özkarataş ŞE, et al. Comparison of retrograde intrarenal surgery and percutaneous nephrolithotomy for the treatment of renal stones greater than 2 cm. Urology Research & Practice. 2015;41(2):73-7.
- Assimos D, Krambeck A, Miller NL, Monga M, Murad MH, Nelson CP, et al. Surgical Management of Stones: American Urological Association/Endourological Society Guideline. The Journal of Urology. 2016;196(4):1153-60.
- InfoSehat FKUI. Fakultas Kedokteran UI. 2023. Guru Besar UI Dorong Transplantasi Ginjal untuk Pengobatan Tahap –Akhir: Lebih Murah dan Kualitas Hidup Lebih Baik. Available from: https://fk.ui.ac.id/infosehat/guru-besar-ui-dorong-transplantasi-ginjal-untuk-pengobatan-tahap-akhir-lebih-murah-dan-kualitas-hidup-lebih-baik.
- Firdaus A. ANTARA: Kantor Berita Indonesia. 2023. Kemenkes: 12 provinsi RI tempati angka tertinggi kasus ginjal kronis. Available from: https://www.antaranews.com/berita/3429303/kemenkes-12-provinsi-ri-tempati-angka-tertinggi-kasus-ginjal-kronis.
- Stamatelou K, Goldfarb DS. Epidemiology of Kidney Stones. Healthcare. 2023;11(3):1-25.
- Chen Z, Prosperi M, Bird VY. Prevalence of kidney stones in the USA: The National Health and Nutrition Evaluation Survey. Journal of Clinical Urology. 2018;12(4):296-302.
- Moftakhar L, Jafari F, Johari MG, Rezaeianzadeh R, Hosseini SV, Rezaianzadeh A. Prevalence and risk factors of kidney stone disease in population aged 40–70 years old in Kharameh cohort study: a cross-sectional population-based study in southern Iran. BMC Uro–logy. 2022;22(1):1-9.
- Kumar S, Karthikeyan VS, Mallya A, Keshavamurthy R. Outcomes of second-look percutaneous nephrolithotomy in renal calculi — a single centre experience. Turkish Journal of Urology. 2018;44(5):406-10.
- Reimer RP, Klein K, Rinneburger M, Zopfs D, Lennartz S, Salem J, et al. Manual kidney stone size measurements in computed tomography are most accurate using multiplanar image reformatations and bone window settings. Scientific Reports. 2021;11(1):1-7.
- Doykov M, Kostov G, Doykova K. Factors Affecting Residual Stone Rate, Operative Duration, and Complications in Patients Undergoing Minimally Invasive Percutaneous Nephrolithotomy. Medi–cina. 2022;58(3):1-12.
- Sabler IM, Katafigiotis I, Gofrit ON, Duvdevani M. Present indications and techniques of percutaneous nephrolithotomy: What the future holds? Asian Journal of Urology. 2018;5(4):287-94.
- Thapa BB, Niranjan V. Mini PCNL Over Standard PCNL: What Makes it Better? The Surgery Journal. 2020;6(1):19-23.
- Wishahi M, Feel A El, Elkhouly A, Fahmy A, Roshdy M, Elbaz AG, et al. Concerns about stone free rate and procedure events of percutaneous nephrolithotripsy (PCNL) for 2–4 cm kidney stones by standard-PCNL vs mini-PCNL comparative randomised study. BMC Urology. 2023;23(1):1-7.
- Atmoko W, Birowo P, Rasyid N. Factors affecting stone free rate of primary percutaneous nephrolithotomy on staghorn calculi: a single center experience of 15 years. F1000Research. 2016;5.
- Chen P, Wei TTC, Huang EYH, Lin TP, Huang TH, Lin CC, et al. Comparison of stone-free rate between percutaneous nephrolithotomy and retrograde intrarenal surgery. Journal of the Chinese Medical Association. 2023;86(5):485-8.