Резюме
У статті детально описаний клінічний випадок рецидивуючого паротиту в 6-річної дитини, наведено результати лабораторного й інструментального обстеження, методи та ефективність терапевтичного підходу. Проведено аналіз і класифікацію можливих інфекційних та неінфекційних причин ураження слинних залоз у дітей, включаючи запальні захворювання, автоімунні та гіпертрофічні ураження, обструктивні та травматичні стани, дефекти розвитку, пухлини. Як приклад наведено діагностичні критерії синдрому Шегрена, саркоїдозу, хвороби кошачих подряпин, кон’юнктивіту Паріно. У результаті диференціального підходу в цьому клiнiчному випадку було встановлено діагноз виключення — ювенільний рецидивуючий паротит. У статті наведено епідеміологічні особливості цієї патології, діагностичні критерії, обговорено можливi причини, рекомендації щодо лікування. Акцент зроблено на необхідності та безпецi вакцинації проти епідемічного паротиту, на важливості уникнення призначення ліків, що не є необхідними. Лікування має бути лише симптоматичним. Підкреслено необхідність подальшого спостереження за пацієнтами після перших епізодів рецидивуючого паротиту.
В статье подробно описан клинический случай рецидивирующего паротита у 6-летнего ребенка, представлены результаты лабораторного и инструментального обследования, методы и эффективность терапевтического подхода. Проведены анализ и классификация возможных инфекционных и неинфекционных причин поражения слюнных желез у детей, включая воспалительные заболевания, аутоиммунные и гипертрофические поражения, обструктивные и травматические состояния, дефекты развития, опухоли. В качестве примера приведены диагностические критерии синдрома Шегрена, саркоидоза, болезни кошачьей царапины, конъюнктивита Парино. В результате дифференциального подхода в данном клиническом случае был поставлен диагноз исключения — ювенильный рецидивирующий паротит. В статье представлены эпидемиологические особенности этой патологии, диагностические критерии, обсуждены возможные причины, рекомендации по лечению. Акцент сделан на необходимости и безопасности вакцинации против эпидемического паротита, на важности избегания назначения ненужных лекарственных средств. Лечение должно быть лишь симптоматическим. Подчеркивается необходимость последующего наблюдения за пациентами после первых эпизодов рецидивирующего паротита.
Currently, with introduction of vaccination against epidemic parotitis, differential diagnosis of salivary gland involvement in children should include other viruses, such as cytomegalovirus, Coxsackie virus, herpes virus type 6, human T-lymphotropic virus, human immunodeficiency virus, etc., as well as autoimmune and oncologic diseases. Comprehensive differential diagnosis is required before establishing the diagnosis of exclusion, such as juvenile recurrent parotitis. It will ensure more effective therapeutic approach and avoiding the prescription of unnecessary medicines and manipulations. The article presents detailed clinical case of recurrent parotitis in a fully vaccinated (according to national vaccination schedule) 6-year-old boy, who experienced several episodes of painless swelling of the left parotid area without fever or with low-grade fever accompanied by redness in the left eye during observation. Performed laboratory survey and instrumental examination are given. Methods and efficacy of therapeutic approach are described. The article presents etiological classification of salivary gland involvement, which includes inflammatory diseases, autoimmune and hypertrophic lesions, obstructive and traumatic conditions, developmental defects, tumors. Epidemiologic and etiologic features of parotitis in pediatric population are considered. Differential diagnosis also includes, for example, Sjogren’s syndrome, sarcoidosis, cat-scratch disease, Parinaud conjunctivitis, with description of diagnostic criteria of the mentioned conditions. According to clinicians, juvenile recurrent parotitis was diagnosed in the presented case. The article presents epidemiological features of this pathology, diagnostic criteria, discussion of possible etiology, recommendations for the management. Necessity and safety of vaccination against epidemic parotitis were accentuated, as well as importance of avoiding the prescription of unnecessary medicines. Vaccination against epidemic parotitis is a prerequisite for the prevention of viral lesions of the salivary glands. It also helps to narrow the differential diagnosis of parotitis causes. If diagnosis of epidemic parotitis is excluded in a child, comprehensive clinical, laboratory and instrumental examination is recommended. It is very important to provide follow-up after the first episode of parotitis in order to exclude recurrent course of the disease. In the presence of recurrent parotitis and exclusion of other causes of damage to the parotid salivary gland, it should be suggested that the child has juvenile recurrent parotitis, which is a diagnosis of exclusion, and can be made after at least 12 months of follow-up. The drug management of juvenile recurrent parotitis should exclude unreasonable prescription of medicines, such as antibiotics, antiviral drugs and especially immunomodulators. Only symptomatic therapy is indicated, providing relief of symptoms. Systematic follow-up of patients with this pathology is required.
Definition
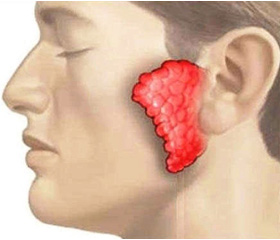
Parotitis is a polyetiological inflammation of the parotid salivary gland clinically manifested by one- or two-sided painful swelling in the parotid region of the face, and accompanied by disturbances of salivation.
Importance
Pre-vaccination era of mumps ended in 1968, when Maurice Hilleman (1919–2005) [1] developed a live vaccine based on the attenuated Jeryl Lynn strain isolated from the saliva of his daughter sick with mumps. In this era, the most common salivary gland (SG) pathology was epidemic parotitis (EP). Currently, despite all the difficulties of immunization in Ukraine, the incidence of EP is sporadic. In this regard, the etiological structure of the causes of SG damage has significantly changed and nowadays can be determined by other viral agents (Table 1), as well as be a manifestation of autoimmune and oncologic diseases. Thus, the pathology of SG in children has its own characteristics and presents an interdisciplinary problem requiring the participation of many specialists.
Clinical observation
Child V., 6-year-old boy, was brought to the clinic of infectious diseases by his parents on February 17, 2016, with complaints of swelling in the left side of the cheekbone and neck, as well as mild fatigue.
Anamnesis morbi. The child became acutely ill three days ago (February 15, 2016), with the appearance of painless swelling in the left parotid region, satisfactory general state and no fever. On the second day, a painless redness appeared in the left eye, due to which pa–rents sought advice from pediatrician who suggested the diagnosis of epidemic parotitis and sent the child to a consultation in an infectious hospital. The boy’s parents do not associate this condition with anything, the last acute disease in the form of acute respiratory infection was in January 2014. However, according to the parents, a state suspicious for parotitis occurred a few months earlier: swelling and tenderness in the outer margin of the left zygomatic bone, accompanied by a short, low-grade fever. They did not apply for medical assistance, since this condition disappeared in a few days without consequences.
Anamnesis vitae. An ethnic Ukrainian, first-grade pupil of the secondary school in Dnipro. The child is not known to have any chronic diseases. Parents deny any allergy in the past. The child is vaccinated according to the national vaccination schedule. The Mantoux test is negative. Family history for any autoimmune diseases is negative according to parents’ statement.
Epidemiological anamnesis. The child did not leave the city within one month. Over the previous three weeks, there was no known contact with EP patients or with persons who had neck swelling. In addition, during the previous month the boy had numerous contacts with domestic and stray cats.
Clinical status at admission. The child is mildly ill, complaining of swelling in the submaxillary region of the face, without signs of general intoxication. The state of health is satisfactory, sleep and appetite are not disturbed. Physical development is normal, nutrition — sati–sfactory. The body temperature in the axillary region throughout the stay in the hospital fluctuated within the physiological norm. There is no rash or itching of the skin. On physical examination, follicular conjunctivitis of the left eye is detected, without signs of exudation and ulceration. Preauricular, submandibular and posterior cervical lymph nodes are enlarged. They are painless on palpation, mobile, of elastic consistency, size: preauricular — 1 × 1 cm, submandibular and posterior cervical — 1.5 × 2 cm. In the left parotid region, there is a dense, painless infiltration, the overlying skin is unchanged. On examination of the oral cavity, there is a slight swelling and hyperemia of the opening of the Steno’s duct detected on the left side of the mucosa (Nicolas Steno, 1638–1686). On the mucosa of the right cheek, there are no changes in the salivary Steno’s duct opening. Physical examination revealed no disturbances of cardiopulmonary and digestive systems. The liver and spleen are not enlarged. Psychoneurological status was with no abnormalities (consciousness by the Glasgow Coma Scale is 15 points). Physiological functions are normal.
Results of laboratory tests. Complete blood count: Нb — 140 g/l, RBC — 4.0 • 1012/l, bands — 6 %, segments — 55 %, eos. — 6 %, lymph. — 31 %, virocytes — 1 %, ESR — 6 mm/h. Urinalysis is without pathology. Bacteriological culture from nasopharynx is negative. According to the results of the serological examination by the enzyme-linked immunosorbent assay, IgM antibodies to Epstein-Barr virus viral capsid antigen (VCA) were not detected, and IgM antibodies to Epstein-Barr virus-associated nuclear antigen (EBNA) were found. Immunobiochemical blood test showed that the level of C-reactive protein was 12 mg/l (normal range is up to 10 mg/l).
Given the clinical examination and the results of laboratory studies, the following clinical diagnosis was established: left-sided nonspecific parotitis; exclude melanosis, conjunctivitis of Parinaud (Henri Parinaud, 1844–1905). Based on the established clinical diagnosis, the boy was prescribed the following therapy: azithromycin PO at a dose of 10 mg/kg once a day, strictly at the same time, for 5 days. Locally — eye drops containing ofloxacin (floxal), 1 drop in the affected eye, 4 times a day. Restrictions in the diet were not prescribed, moreover, the use of chewing gum is recommended to improve the outflow of saliva. The therapy had positive effect, and the child was discharged from the department in satisfactory condition for further supervision by his family doctor. A month and a half after discharge from the hospital, the child’s parents applied to the hospital again complaining of swelling and tenderness in the left parotid region when chewing, short-term low-grade fever, mild fatigue. To determine the causes of the current parotid enlargement, ultrasound examination of the parotid and submandibular regions was performed, which revealed an increase in the left parotid gland size due to diffuse edema of the tissues. Concrements or tumors were not found. The child was prescribed: ibuprofen PO, oral hygiene in the form of mouth washing, solid food, use of a soft chewing gum. It was decided to refuse antibiotics. The clinical signs disappeared within few days. The boy’s parents were given the following recommendations: 1) to seek medical help immediately, if there is another one episode of swelling in the submandibular or parotid region; 2) to continue periodical mouth washing, include foods that require a thorough chewing (apples, carrots, bagels, etc.). During the follow-up, which was about 2 years by the moment of the article writing, there were no repeated episodes of SG enlargement in this boy.
Discussion
The feature of the presented case was the recurrence of parotid gland enlargement within one year. Swelling in the parotid and/or submandibular region of the neck may be caused by the lesion of one of the three anatomical areas: SG disease, lymphadenitis/lymphadenopathy and purulent-septic processes in the muscles of mastication, for example, the so-called Ludwig’s angina (Wilhelm Frederick von Ludwig, military doctor in the army of Napoleon, 1790–1865). The most appropriate classification of SG diseases answers the practical question: “Who and where should treat the problem?” and is based on etiopathogenetic principle (Table 2).
/130-1.jpg)
In children, the ratio of lesions (on average, for all pathologies) of the parotid, submaxillary and sublingual gland is 30 : 6 : 1 [3]. According to the disease semio–tics, the anamnesis, as well as the results of laboratory and instrumental studies, in all episodes the boy appa–rently had a lesion of parotid gland. Thus, from the point of view of the anatomical locus of inflammation, the di–sease (parotitis) was diagnosed, but from the standpoint of etiology, the causes of recurrent mumps were not fully established.
The presence of any recurring process, including parotitis, suggests an extensive spectrum of differential diagnosis of the causes of parotid enlargement. Based on the results of serological tests (absence of VCA-IgM antibodies, which are the marker of the acute phase of the infectious process, and the presence of EBNA-IgG, which is typical of the post-infection stage), the herpesviral Epstein-Barr infection was excluded in the child as a possible cause of enlarged lymph nodes and SG. One of the significant defects in clarifying the causes of a recurrent enlargement of SG, in our opi–nion, was the parents’ refusal to perform HIV testing of the child. The recurrent enlargement of SG without significant clinical signs of the infectious process also requires the exclusion of non-infectious etio–logy of parotitis, and most notably: Sjogren’s disease/syndrome (Henrik Sjögren, 1899–1986), sarcoidosis (Heerfordt syndrome), Mikulicz disease, swelling and sialolithiasis [4, 5]. Sjogren’s syndrome is a systemic autoimmune disease, which is one of the most common causes of SG lesion in adults. In pediatric practice, Sjogren’s syndrome is a very rare disease: only 145 cases have been described in the world literature, and the ratio of boys to girls is 1 : 6 [6, 7]. According to the American-European classification group (AECG), Sjögren’s syndrome is determined by the following parameters (Table 3) [8].
/131-1.jpg)
Given the benign nature of SG lesions and the absence of extra-glandular lesions of a systemic nature, the diagnosis of Sjogren’s syndrome is excluded at this stage. However, it should be noted that the long-term, recurrent parotitis in childhood can be one of the risk factors for the development of this autoimmune disease, the peak of Sjogren’s syndrome onset falls on the 4th — 5th decades of life [9]. Neoplastic processes in the SG are relatively rare and in general they account for 5–6 % of all head and neck tumors in children and adults [10, 11]. At the same time, at any age most tumors are located in the parotid gland [3, 13]. It should be noted that the absence of pain and fever indicated the risk of SG tumor. However, parotitis regression, SG elasticity, and intact VII (n.facialis) pairs of cranial nerves exclude malignant process in the described clinical case.
The presence of parotitis episodes with conjunctivitis and enlargement of regional lymph nodes may be a manifestation of sarcoidosis. One of the main symptoms occurring in sarcoidosis is Heerfordt syndrome (syn.: uveopa–rotitis, neurouveoparotitis, uveomeningitis, uveoparotitis fever, Heerfordt-Mylius syndrome). This di–sease was described in 1909 by Christian Frederik Heerfordt (1871–1953), an ophthalmologist from Denmark [14]. However, absence of facial nerve or respiratory tract involvement, as well as the presence of ophthalmic manifestations, exclusively in the form of conjunctivitis, without signs of uveitis/iridocyclitis or optic neuritis, allow excluding sarcoidosis. Furthermore, Heerfordt syndrome is described in adulthood, mainly in females [15]. It should be noted that the combination of parotitis with enlarged preauricular lymph nodes and conjunctivitis, and possible contact with kittens, suggests that one of parotitis episodes could be caused by zoonotic infection with Bartonel–la henselae. The sources of infection with B.henselae are stray and domestic cats (predominantly kittens), which gave it the name — cat-scratch disease. The disease is characterized by regional lymphadenitis/lymphadenopathy, possible suppurating papules in the scratch site, and in some cases — conjunctivitis, if the infection site was the face of what is described as Pari–naud conjunctivitis. This group of symptoms should not be confused with yet another neurological eponym, named Parinaud, associated with damage to the midbrain structures. Cat-scratch disease in immunocompetent indivi–duals is a benign disease resul–ting in most cases in complete recovery, which is indirectly confirmed by the results of serological tests — 37 % of those specific antibodies to B.henselae were found in the general population. Obturative genesis of parotitis due to sialolithiasis was excluded by ultrasound, which showed the absence of concrements and tumor formations in the salivary ducts.
In our opinion, repeated episodes of parotid swelling, with the exclusion of other causes, may be induced by juvenile recurrent parotitis (JRP). This state is defined as idiopathic, benign, non-obstructive, non-purulent, relapsing parotid disease in children, self-limiting in puberty age [3, 12, 16, 17]. Information about the prevalence of this disease in pediatric practice is very contradictory, because there is no generally accepted statistics, but, according to the literature, it varies from 1.1 to 1.9 % among children under sixteen [18]. The generally accepted diagnostic criteria for the JRP, in addition to the fact that it must be exclusively children under 16 years of age, are the following [18, 19]:
1. Recurring episodes of sudden onset of parotid salivary edema with/without pain associated with fever and weakness, which can persist from day to 2 weeks.
2. The course of parotitis is benign, it resolves spontaneously by 16–18 years of age.
3. After the first episode, there is a period of well-being followed by longer episodes. The natural history of this disease suggests sometimes up to 20 episodes of SG enlargement per year.
4. There is a gender dependence (boys prevail), and it occurs after 3 months of life.
5. More often, unilateral involvement of SG is described.
The first two of the above-mentioned criteria are pathognomonic, the rest characterize the most common signs of the disease [4, 11, 16, 17].
As said above, JRP is an idiopathic disease. As probable causes, factors such as autoimmune disorders, congenital malformations of the salivary ducts, hereditary diseases, allergies, repeated bacterial or viral infections were considered [19]. The JRP can be classified as the so-called diagnosis of exclusion, since it is made when all the above-mentioned conditions are excluded, and after a rather long period of follow-up. In the treatment of JRP, polypharmacy should be avoided, especially unreasonable use of systemic antibacterial and antiviral chemotherapy, various immunomodulators are stricktly prohibited, there are no contraindications to immunoprophylaxis with all kinds of vaccines. This pathology requires only symptomatic therapy: oral hygiene, non-steroidal anti-inflammatory drugs (ibuprofen or paracetamol) and the use of chewing gum.
Practical recommendations
1. Vaccination against the mumps virus is a prere–quisite for the prevention of viral lesions of the SG and narrowing the differential diagnosis of parotitis causes.
2. In case of the first episode of SG enlargement and the exclusion of the epidemic parotitis virus, the child is required comprehensive clinical, laboratory and, if ne–cessary, instrumental examination to exclude other causes of SG damage.
3. In the presence of recurrent parotitis and if –other causes of damage to the parotid SG are excluded, it should be suggested that the child has JRP, which is a diagnosis of exclusion made after at least 12 months of follow-up.
4. Systematic follow-up of patients with diagnosed juvenile recurrent parotitis is recommended for several years to evaluate recurrence pattern in a specific patient.
5. Drug management of juvenile recurrent parotitis should exclude unreasonable prescription of medicines, such as antibiotics, antiviral drugs and especially immunomodulators, as they provide no therapeutic benefit to minimal symptomatic therapy.
Conflicts of interests. Authors declare no conflicts of interests that might be construed to influence the results or interpretation of their manuscript.
Список литературы
1. Маврутенков В.В. Вакцинопрофілактика: досягнення, проблеми і перспективи розвитку / Маврутенков В.В., Ревенко Г.О. // Медичні перспективи. — 2016. — Т. ХХІ, № 3. — C. 56-60.
2. Juvenile parotitis. Riitta Saarinen / University of Helsinki Faculty of Medicine Helsinki 2012 academic dissertation. Available from: https://helda.helsinki.fi/bitstream/handle/10138/36427/juvenile.pdf?sequence=1
3. Sunday Olusegun Ajike, Kokila Lakhoo. Ch. 39. Salivary gland diseases in children and adolescents // Paediatric Surgery: A Comprehensive Text for Africa. Available from: https://storage.googleapis.com/global-help-publications/books/help_pedsurgeryafrica39.pdf
4. Wilson K.F. Salivary gland disorders / Wilson K.F., Meier J.D., Ward P.D. // Am. Fam. Physician. — 2014 Jun. — 89(11). — 882-8.
5. Means C. Pediatric primary Sjögren syndrome presenting with bilateral ranulas: A case report and systematic review of the literature / Means C., Aldape M.A., King E. // Int. J. Pediatr. Otorhinolaryngol. — 2017 Oct. — 101. — 11-19; doi: 10.1016/j.ijporl.2017.07.019. Epub 2017 Jul 19.
6. Civilibal M. A child with primary Sjogren syndrome and a review of the literature / Civilibal M., Canpolat N., Yurt A. et al. // Clin. Pediatr. (Phila). — 2007 Oct. — 46(8). — 738-42.
7. Cimaz R. Primary Sjogren syndrome in the pediatric age: a multicenter survey / Cimaz R., Casadei A., Rose C. et al. // Eur. J. Paediatr. — 2003. — 162(10). — 661-5.
8. Vitali C. et al. Classification criteria for Sjogren’s syndrome: a revised version of the European criteria proposed by the American-European Consensus Group // Ann. Rheum. Dis. — 2002. — 61. — 554-558.
9. Recurrent parotitis as a presentation of primary pediatric Sjögren Syndrome // Pediatrics. — 2012. — 129. — e179; naturally published online December 19, 2011; doi: 10.1542/peds.2011-0716.
10. Stenner M. Current update on established and novel biomarkers in salivary gland carcinoma pathology and the molecular pathways involved / Stenner M., Klussmann J.P. // Eur. Arch. Otorhinolaryngol. — 2009 Mar. 266(3). — 333-41.
11. Robert A. Ord. Pediatric salivary gland malignancies / Ro–bert A. Ord, Eric R. Carlson // Oral Maxillofacial Surg. Clin. N. Am. — 2016. — 28. — 83-89.
12. Tomar R.P.S. Juvenile recurrent parotitis / Tomar R.P.S., Vasudevan R., Manoj K., Gupta D.K. // Med. J. Armed Forces India. — 2014 Jan. — 70(1). — 83-84; doi: 10.1016/j.mjafi.2012.08.013.
13. Hädicke J. Recurrent swelling of parotid gland in children [German] / Hädicke J., Pethe W., Drüg-Skamel S., Begall K. // HNO. — 2015 Jul. — 63(7). — 520-2; doi: 10.1007/s00106-015-0026-5.
14. Heerfordt C. Uber eine Febris uveo-parotidea subchronica // Von Graefe’s Archiv fur Opthalmologie — 1909. — 70. — 254-73.
15. Tiia Tamme. Sarcoidosis (Heerfordt syndrome): A case report / Tiia Tamme, Edvitar Leibur, Andres Kulla // Stomatologija. Baltic Dental and Maxillofacial Journal. — 2007. — 9(2). — 61-64.
16. Schorr B. Diagnosing juvenile recurrent parotitis. Case reports / Schorr B., Mandel L. // N.Y. State Dent. J. — 2016 Jan. — 82(1). — 36-9.
17. Saarinen R. The clinical picture of juvenile parotitis in a prospective setup / Saarinen R., Kolho K.L., Davidkin I., Pitkäranta A. // Acta Paediatr. — 2013 Feb. — 102(2). — 177-81; doi: 10.1111/apa.12004. Epub 2012 Sep 17.
18. Sujatha S. Case report: Report of a rare case of juvenile recurrent parotitis and review of literature / Sujatha S., Rakesh N., Raghav N., Devaraju D., Shridevi G. // Eur. Arch. Paediatr. Dent. — 2009 Nov. — 10, Suppl. 1. — 31-4.
19. Clinical practice guideline for salivary gland disorders. Develo–ped for the Aerospace Medical Association by their constituent organization American Society of Aerospace Medicine Specia–lists. Available from: http://www.asams.org/guidelines/Completed/NEW%20Salivary%20Gland%20Disorders.htm

/129-1.jpg)