Резюме
Актуальність. Ураження суглобів є однією з типових і часто перших ознак системного червоного вовчака (СЧВ) й спостерігається майже в 90 % пацієнтів як у дебюті, так і впродовж захворювання. При цьому особливості клінічних і лабораторних змін у хворих без залучення суглобів залишаються недостатньо вивченими. Мета — вивчити частоту суглобового синдрому у хворих на СЧВ та оцінити його зв’язок з клініко-лабораторними проявами захворювання. Матеріали та методи. Проаналізовано дані 376 хворих з діагнозом СЧВ, серед яких 325 жінок (86,4 %) та 51 чоловік (13,6 %). Сформовано 2 групи хворих: І — із суглобовим синдромом у вигляді артриту та/або артралгій на момент звернення (n = 316), ІІ — без суглобового синдрому (n = 60). Проведено оцінку залучення різних органів і систем, а також рівнів маркерів запалення та спектра специфічних автоантитіл. Результати. У хворих на СЧВ із суглобовим синдромом значно частіше (34,1 проти 20,0 %, p = 0,04) спостерігали еритематозний висип на обличчі у вигляді «метелика». Ураження серозних оболонок частіше мало місце у хворих на СЧВ із суглобовим синдромом (39,6 %), ніж у пацієнтів без нього (25,4 %, р = 0,048). Нефрит з нефротичним синдромом у 4 рази частіше спостерігали у хворих на СЧВ без артритів/артралгій порівняно з пацієнтами із суглобовим синдромом (10,2 проти 2,6 %, p = 0,04). Частота антифосфоліпідного синдрому також була значно вищою у хворих на СЧВ без суглобового синдрому (25,5 проти 6,0 %, p < 0,001). Група хворих на СЧВ із суглобовим синдромом мала більшу, ніж група хворих без ураження суглобів, частоту синдрому Рейно (27,5 проти 15,0 %, p = 0,046), лімфаденопатії (50,5 проти 35,6 %, p = 0,048), ураження серця (62,5 проти 42,4 %, р = 0,007), схуднення (13,6 проти 3,8 %, р = 0,04) та позитивності за антитілами до двоспіральної ДНК (65,0 проти 45,7 %, р = 0,03). Значення індексу активності СЧВ SLEDAI було вірогідно вищим у хворих на СЧВ із наявним суглобовим синдромом (11 (6–16) проти 7,5 (4–14) бала, р = 0,01). Хворі на СЧВ із суглобовим синдромом отримували вірогідно вищі дози пероральних глюкокортикоїдів (10 (10–20) мг/д у преднізолоновому еквіваленті) порівняно з пацієнтами без м’язово-скелетних проявів (6,25 (3,75–12,5) мг/д, р = 0,01). Висновки. Висип на обличчі у вигляді «метелика», серозити, ураження серця, лімфаденопатія, синдром Рейно, схуднення та позитивність за антитілами до двоспіральної ДНК вірогідно частіше спостерігаються у хворих на СЧВ із суглобовим синдромом. Водночас нефрит з нефротичним синдромом та антифосфоліпідний синдром частіше мають місце у хворих на СЧВ без ураження суглобів. Суглобовий синдром у хворих на СЧВ асоціюється з вищим індексом активності захворювання та потребою у більш високих дозах глюкокортикоїдів.
Background. Damage of the joints is one of the typical and often the first signs of systemic lupus erythematosus (SLE), however the peculiarities the of clinical and laboratory changes in patients without articular manifestations (AM) remain insufficiently studied. The purpose was to study the frequency of AM in the patients with SLE and to evaluate its interconnection with clinical and laboratory manifestations of the disease. Materials and methods. 376 patients with SLE were examined. 2 groups were formed: I — with AM presented as arthritis and/or arthralgia at the time of application (n = 316), II — without AM (n = 60). The involvement of various organs and systems, as well as the levels of inflammatory markers and the spectrum of specific autoantibodies, were evaluated. Results. Patients with SLE and AM had erythematous rash on the face in the form of a “butterfly” more often than the patients without AM (34.1 vs. 20.0 %, p = 0.04). Serositis was more often observed in patients with AM (39.6 %) compared to the patients without AM (25.4 %, p = 0.048). Nephritis with nephrotic syndrome was 4 times more frequent in patients without arthritis/arthralgia compared to the subjects with AM (10.2 vs. 2.6 %, p = 0.04). The frequency of antiphospholipid syndrome was also significantly higher in patients without AM (25.5 vs. 6.0 %, p < 0.001). The group of the patients with SLE and AM had a higher frequency of Raynaud’s syndrome (27.5 vs. 15.0 %, p = 0.046), lymphadenopathy (50.5 vs. 35.6 %, p = 0.048), heart involvement (62.5 vs. 42.4 %, p = 0.007), weight loss (13.6 vs. 3.8 %, p = 0.04) and positivity for antibodies to dsDNA (65.0 vs. 45.7 %, p = 0.03), than the patients without AM. The median value of SLEDAI was significantly higher in the patients with SLE and AM (11 (6–16) points vs. 7.5 (4–14) points, р = 0.01). Also they received significantly higher doses of oral glucocorticoids (10 (10–20) mg/d in prednisolone equivalent) compared to the subjects without AM (6.25 (3.75–12.5) mg/d, p = 0.01). Conclusions. Rash on the face in the form of a “butterfly”, serositis, heart involvement, lymphadenopathy, Raynaud’s syndrome, weight loss, and anti-dsDNA positivity are significantly more common in SLE patients with AM. Nephritis with nephrotic syndrome and antiphospholipid syndrome occur more often in patients with SLE without AM. Presence of arthritis/arthralgia in patients with SLE is associated with a higher index of disease of activity and the need for higher doses of glucocorticoids.
Вступ
Ураження опорно-рухового апарату є одним із найбільш частих проявів системного червоного вовчака (СЧВ) і спостерігається в 65–95 % пацієнтів у дебюті або впродовж захворювання [1]. Суглобовий синдром при СЧВ характеризується значною гетерогенністю, починаючи від артралгій і артриту без деформацій суглобів до артропатії Жаку та навіть ерозивного артриту [2]. Частіше зустрічаються артралгії, які проявляються транзиторним і мігруючим болем у суглобах, переважно кистей, іноді з нетривалою ранковою скутістю без ознак набряку в суглобах [3].
Артрит при СЧВ переважно є неерозивним і симетричним, з ураженням дрібних суглобів кистей, променево-зап’ясткових і колінних суглобів [3]. Він традиційно розцінюється як легкий прояв захворювання, що не потребує агресивного лікування. І хоча артрит не належить до станів, загрозливих для життя, м’язово-скелетні прояви значно погіршують якість життя хворих на СЧВ [1, 4, 5].
Вважається, що ерозивні кісткові зміни при СЧВ виникають у пацієнтів із супутнім переважно серопозитивним ревматоїдним артритом (РА), що класифікується як rhupus-синдром. Пацієнти з цим синдромом відповідають класифікаційним критеріям одночасно СЧВ та РА і становлять 3–5 % хворих на СЧВ із суглобовим синдромом [6].
Літературні дані щодо ураження суглобів при СЧВ переважно акцентують увагу на артропатії Жаку, яка виникає внаслідок ураження періартикулярних тканин і є порівняно рідкісним проявом [7, 8]. Деякі дослідники твердять, що артропатія Жаку асоціюється з вищою частотою синдрому Шегрена й нижчою частотою ураження нирок [9, 10], інші автори не знаходять таких асоціацій [8, 11]. P.E. Spronk та співавт. у своєму дослідженні описують асоціацію артропатії Жаку з підвищеним рівнем С-реактивного білка [12]. Кілька публікацій вказують на асоціацію артропатії Жаку з позитивністю за антитілами до двоспіральної ДНК (АТ-дсДНК) [9, 10] або антитілами до Ro/SS-A [7]. R.M. Van Vugt та співавт. виявили зв’язок між артропатією Жаку та антифосфоліпідними антитілами й припустили, що тромбоз дрібних судин може викликати ішемію та навколосуглобовий фіброз [13]. Натомість практично не дослідженим залишається питання, чи взагалі асоціюється наявність суглобового синдрому (у вигляді артралгій та/або артритів) у хворих на СЧВ з іншими клініко-лабораторними проявами захворювання. Нами також не знайдено літературних даних з результатами вивчення цього питання на українському контингенті хворих на СЧВ.
Мета роботи: вивчити частоту суглобового синдрому у хворих на СЧВ та оцінити його зв’язок з клініко-лабораторними проявами захворювання.
Матеріали та методи
В одномоментному одноцентровому дослідженні проаналізовано дані 387 хворих з діагнозом СЧВ відповідно до критеріїв EULAR/ACR (2019) [14], які спостерігались на кафедрі внутрішньої медицини № 3 Національного медичного університету імені О.О. Богомольця в період з 1994 до 2022 року. Усім хворим, які первинно потрапили під спостереження до 2019 року, діагноз встановлювали відповідно до критеріїв ACR (1982, оновлені 1997) [15], у 2019 р. діагноз СЧВ у цих хворих було переглянуто на предмет відповідності критеріям EULAR/ACR. За результатами такого перегляду з первинного пулу хворих було виключено 11, в остаточний аналіз включено дані 376 осіб. Дослідження проводили відповідно до умов Гельсінської декларації за схвалення Комісії з питань біоетичної експертизи при НМУ імені О.О. Богомольця (протокол № 127 від 02.12.2019 р).
Було сформовано 2 групи хворих: І — із суглобовим синдромом (n = 316), ІІ — без суглобового синдрому (n = 60). Під суглобовим синдромом розуміли наявність артралгій (як правило, поліартралгій) та/або візуалізованих за допомогою ультразвукового чи магнітно-резонансно-томографічного дослідження артритів, які хронологічно збігалися з часом розвитку інших симптомів СЧВ та не мали інших зрозумілих причин. Особи обох груп вірогідно не відрізнялись за показниками віку (36 (25,5–48) проти 36,5 (25,5–46) року, р = 0,98), статі (частка жінок 86,7 проти 85,0 % чоловіків, р = 0,88) та тривалості захворювання (55 (23–120) проти 50 (10–132) місяців, р = 0,59).
Проведено кількісну та якісну оцінку залучення різних органів і систем з визначенням індексів активності (SLEDAI) [16] та пошкодження (SLICC/DI) [17], а також оцінку рівнів маркерів запалення (швидкість осідання еритроцитів (ШОЕ), С-реактивний білок (СРБ)) та спектра специфічних для СЧВ автоантитіл. ШОЕ визначали за Вестергреном, сироватковий рівень СРБ — аглютинаційним та імуноферментним (з використанням тест-систем фірми DRG International Inc., США) методами, антинуклеарний фактор (АНФ) та АТ-дсДНК, антитіла до антигенів Sm, Ro/SSA, La/SSB, рибонуклеопротеїну (RNP), а також антифосфоліпідні антитіла (АФЛ-АТ) — методом імуноферментного аналізу. АНФ визначали в усіх хворих, спектр автоантитіл — у 266 хворих (70,7 %).
Статистичну обробку результатів проводили за допомогою ліцензійних програм Microsoft Excel та SPSS. Для подання кількісних показників розраховували медіанне значення та значення першого й третього квартилей (Me (QI–QIII)), якісних даних — абсолютні значення (n), частоту (%) та 95% довірчий інтервал (95% ДІ). Для оцінки значущості різниці медіанних значень у досліджуваних групах використовували непараметричний критерій Вілкоксона — Манна — Уїтні. Для визначення відповідності (узгодженості чи відмінності) розподілу показників (частоти виявлення) у досліджуваних групах використовували критерій χ2 (з урахуванням поправки на безперервність — поправки Єйтса). Його розрахунок здійснювали за чотирьохпольною таблицею згідно зі встановленою формулою [18]. Відмінності вважали вірогідними за р < 0,05.
Результати
Серед включених в аналіз пацієнтів було 325 жінок (86,4 %) та 51 чоловік (13,6 %). Вік хворих становив у середньому 36 (25,5–48) років, тривалість захворювання — 51 (22–120) місяць. Вік хворих на момент дебюту захворювання становив 25 (19–38) років. У дослідженні брали участь хворі переважно з хронічним перебігом захворювання (84,8 %). Низька активність СЧВ (індекс SLEDAI 0–5 балів) спостерігалась у 82 хворих (21,8 %), середній ступінь активності (індекс SLEDAI 6–10 балів) — у 110 пацієнтів (29,3 %), високий ступінь активності захворювання (індекс SLEDAI більше ніж 10 балів) — у 184 хворих (48,9 %). Індекс активності SLEDAI становив 10 (6–16) балів, індекс ушкодження SLICC — 1 (0–2) бал. На момент включення в дослідження 44,4 % хворих отримували амінохінолінові препарати, 59,3 % — пероральні глюкокортикоїди (ГК), 12,8 % — пульс-терапію ГК, 2,1 % — циклофосфамід, 2,1 % — метотрексат, 1,2 % — азатіоприн, 0,8 % — мікофенолату мофетил. Середня добова доза ГК за пероральним преднізолоном на момент обстеження становила 10 (7,5–20) мг.
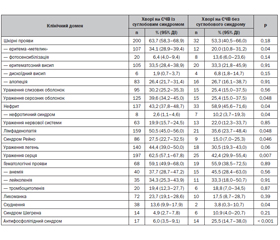
Отримані результати (табл. 1) показують, що у хворих на СЧВ із суглобовим синдромом значно частіше (34,1 проти 20,0 %, p = 0,04) спостерігався еритематозний висип на обличчі у вигляді «метелика». Інші шкірні прояви, зокрема фотосенсибілізація, алопеція, еритематозний і дискоїдний висип, зустрічались з однаковою частотою у хворих незалежно від наявності суглобового синдрому. Не було також виявлено асоціацій між наявністю суглобового синдрому та ураженням слизових оболонок.
/24.jpg)
Ураження серозних оболонок у 1,5 раза частіше спостерігалось у хворих на СЧВ із суглобовим синдромом (39,6 %) порівняно з пацієнтами без м’язово-скелетних проявів (25,4 %, р = 0,048). Натомість частота ураження нирок була вірогідно вищою у хворих на СЧВ без суглобових проявів. Зокрема, нефрит з нефротичним синдромом у 4 рази частіше спостерігався у хворих на СЧВ без артритів/артралгій порівняно з пацієнтами із суглобовим синдромом (10,2 проти 2,6 %, p = 0,04). Схожу закономірність було виявлено щодо антифосфоліпідного синдрому: його частота була значно вищою у хворих на СЧВ без суглобового синдрому (25,5 проти 6,0 %, p < 0,001).
У групі хворих на СЧВ із суглобовим синдромом частіше, ніж у хворих без ураження суглобів, зустрічались синдром Рейно (27,5 проти 15,0 %, p = 0,046), лімфаденопатія (50,5 проти 35,6 %, p = 0,048) та ураження серця (62,5 проти 42,4 %, р = 0,007). Частота схуднення в групі хворих із суглобовим синдромом становила 13,6 %, тоді як у групі без суглобового синдрому — 3,8 % (р = 0,04).
Частота інших клінічних проявів, зокрема уражень нервової системи, легень, лихоманка, гематологічні прояви, синдром Шегрена, вірогідно не відрізнялась між групами.
Значення індексу активності СЧВ SLEDAI було вірогідно вищим у хворих на СЧВ із наявним суглобовим синдромом (табл. 2). Не спостерігалось відмінностей між групами щодо індексу пошкодження SLICC, а також рівнів ШОЕ та СРБ.
Згідно з отриманими даними, наявність суглобового синдрому вірогідно асоціювалась із позитивністю за АТ-дсДНК (табл. 3). У хворих без ураження суглобів дещо частіше виявлялися АФЛ-АТ, проте ця відмінність не досягла статистичної значущості. Статистичних відмінностей між групами щодо позитивності за іншими специфічними автоантитілами (до Sm, Ro/SSA, La/SSB та RNP) виявлено не було.
Також нами виявлено, що хворі на СЧВ із суглобовим синдромом отримували вірогідно вищі дози пероральних ГК (10 (10–20) мг/д у преднізолоновому еквіваленті) порівняно з пацієнтами без ушкодження суглобів (6,25 (3,75–12,5) мг/д, р = 0,01). За частотою прийому пероральних ГК (57,9 проти 58,5 %, р = 0,92), амінохінолінових препаратів (45,5 проти 36,6 %, р = 0,37), метотрексату (2,0 проти 2,4 %, р = 0,65), азатіоприну (1,5 проти 0 %, р = 0,99), мікофенолату мофетилу (0,5 проти 2,4 %, р = 0,78), циклофосфаміду (2,0 проти 2,4 %, р = 0,65), застосування пульс-терапії ГК (11,4 проти 17,1 %, р = 0,47) групи вірогідно не відрізнялись.
Обговорення
За результатами нашого дослідження, суглобовий синдром у вигляді артралгій та/або артритів спостерігався у 84 % хворих на СЧВ, що добре узгоджується з даними інших авторів [1, 6]. Наші результати частково відповідають наявним літературним даним щодо клініко-лабораторних характеристик хворих на СЧВ із суглобовим синдромом, хоча слід брати до уваги, що у проаналізованих публікаціях суглобовий синдром було представлено переважно артропатією Жаку. D. Alargon-Segovia та співавт. відзначали асоціацію суглобового синдрому з позитивністю за АТ-дсДНК [10]. J.F. Molina та співавт. описували асоціацію суглобового синдрому з нижчою частотою ураження нирок, припускаючи, що хворі з ураженням суглобів мають загалом сприятливіший прогноз [10]. Описано також асоціацію між синдромом Рейно і артритом/артралгіями у хворих на СЧВ [19]. На відміну від опублікованих раніше робіт [7, 9, 10, 12] нами не виявлено взаємозв’язку між наявністю суглобового синдрому та синдрому Шегрена, підвищеним рівнем СРБ та позитивністю за АТ-Ro/SS-A. Щодо отриманих нами даних про вищу частоту лімфаденопатії, ураження серця та схуднення у хворих з ураженням суглобів порівняно з альтернативною групою, то їх релевантність неможливо оцінити, оскільки такі взаємозв’язки не вивчались у попередніх дослідженнях. Хоча в поодиноких публікаціях вказують на асоціацію м’язово-скелетних проявів з позитивністю за АФЛ-АТ [13], нами було виявлено вірогідно нижчу частоту антифосфоліпідного синдрому у хворих на СЧВ із суглобовим синдромом, при цьому групи суттєво не відрізнялись за частотою виявлення АФЛ-АТ. У дослідженнях інших авторів не вивчали взаємозв’язок між наявністю суглобового синдрому та величинами індексу активності СЧВ SLEDAI, клінічно необхідними дозами ГК.
Варто зазначити, що виявлена нами на українському контингенті хворих асоціація суглобового синдрому з еритемою «метеликом» та ураженням серозних оболонок підтверджує діагностичну значущість задекларованої раніше класичної клінічної тріади СЧВ (дерматит, артрит, серозит) [20].
Обмеження дослідження. У наше дослідження було включено як медикаментозно наївних пацієнтів, так і хворих, що почали отримувати лікування СЧВ, що могло вплинути на рівень деяких лабораторних показників. Також ми не розділяли хворих на підгрупи залежно від виду суглобового синдрому (артралгії, неерозивний артрит, ерозивний артрит тощо), це питання потребує окремого вивчення.
Висновки
Суглобовий синдром в українській популяції хворих на СЧВ зустрічається у 84 % випадків. Еритематозний висип на обличчі у вигляді «метелика», серозити, ураження серця, лімфаденопатія, синдром Рейно, схуднення та позитивність за АТ-дсДНК вірогідно частіше спостерігаються у хворих на СЧВ із суглобовим синдромом, тоді як нефрит з нефротичним синдромом та антифосфоліпідний синдром частіше мають місце у хворих на СЧВ без ураження опорно-рухового апарату. Суглобовий синдром у хворих на СЧВ асоціюється з вищим індексом активності захворювання та потребою у вищих дозах ГК.
Конфлікт інтересів. Автори заявляють про відсутність конфлікту інтересів та власної фінансової зацікавленості при підготовці даної статті.
Інформація про фінансування. Дослідження є фрагментом науково-дослідної теми кафедри внутрішньої медицини № 3 НМУ імені О.О. Богомольця «Розробка персоніфікованих методів оцінки активності, прогнозування перебігу та відповіді на лікування імуноопосередкованих запальних захворювань» (номер держреєстрації 0121U107784). Установою, що фінансує дослідження, є Міністерство охорони здоров’я України.
Інформація про внесок кожного автора в написання статті. Яременко О.Б. — концепція та дизайн дослідження, відбір пацієнтів, збір даних, аналіз та інтерпретація даних, редагування статті; Коляденко Д.І. — збір та обробка даних, аналіз та інтерпретація даних, аналіз літературних джерел, написання статті.
Отримано/Received 08.10.2022
Рецензовано/Revised 22.11.2022
Прийнято до друку/Accepted 01.12.2022
Список литературы
1. Tomicevic L.S., Hocevar A., Sukara G., Cubelic D., Mayer M. The frequency and characteristics of ultrasonographic ankle joint involvement in systemic lupus erythematosus: A prospective cross-sectional single-center study. Medicine. 2022. 101(31). e29196. doi: 10.1097/md.0000000000029196.
2. Ceccarelli F., Sciandrone M., Perricone C. et al. Biomarkers of erosive arthritis in systemic lupus erythematosus: Application of machine learning models. PLoS One. 2018. 13(12). e0207926. doi: 10.1371/journal.pone.0207926.
3. Ceccarelli F., Perricone C., Cipriano E. et al. Joint involvement in systemic lupus erythematosus: From pathogenesis to clinical assessment. Semin. Arthritis Rheum. 2017. 47(1). 53-64. doi: 10.1016/j.semarthrit.2017.03.022.
4. Zayat A.S., Mahmoud K., Yusof M.Y.M. et al. Defi–ning inflammatory musculoskeletal manifestations in systemic lupus erythematosus. Rheumatology. 2019. 58(2). 304-312. doi: 10.1093/rheumatology/key277.
5. Sippl N., Faustini F., Rönnelid J. et al. Arthritis in systemic lupus erythematosus is characterized by local IL-17A and IL-6 expression in synovial fluid. Clin. Exp. Immunol. 2021. 205(1). 44-52. doi: 10.1111/cei.13585.
6. Ceccarelli F., Natalucci F., Olivieri G. et al. Erosive arthritis in systemic lupus erythematosus: not only Rhupus. Lupus. 2021. 30(13). 2029-2041. doi: 10.1177/09612033211051637.
7. Takeishi M., Mimori A., Suzuki T. Clinical and immunological features of systemic lupus erythematosus complicated by Jaccoud’s arthropathy. Mod. Rheumatol. 2001. 11(1). 47-51. doi: 10.3109/s101650170043.
8. Piga M., Congia M., Balestrieri A. et al. Imbalanced MMP-3 and MMP-12 serum levels in systemic lupus erythematosus patients with Jaccoud’s arthropathy and a di–stinctive MRI pattern. Rheumatology (Oxford). 2021. 60(9). 4218-4228. doi: 10.1093/rheumatology/keaa915.
9. Skare T.L., Godoi Ade L., Ferreira V.O. Jaccoud arthropathy in systemic lupus erythematosus: clinical and serological findings. Rev. Assoc. Med. Bras. 2012. 58(4). 489-92.
10. Santiago M.B. Jaccoud-type lupus arthropathy. Lupus. 2022. 31(4). 398-406. doi: 10.1177/09612033221082908.
11. Santiago M.B., Galvão V. Jaccoud arthropathy in systemic lupus erythematosus: analysis of clinical characteristics and review of the literature. Medicine (Baltimore). 2008. 87(1). 37-44. doi: 10.1097/MD.0b013e3181632d18.
12. Spronk P.E., ter Borg E.J., Kallenberg C.G. Patients with systemic lupus erythematosus and Jaccoud’s arthropathy: a clinical subset with an increased C reactive protein response? Ann. Rheum. Dis. 1992. 51(3). 358-61. doi: 10.1136/ard.51.3.358.
13. Van Vugt R.M., Derksen R.H.W.M., Kater I., Bijlsma J.W.J. Deforming arthropathy or lupus and lupus hands in systemic lupus erythematosus. Ann. Rheum. Dis. 1998. 57. 540-4.
14. Aringer M. EULAR/ACR classification criteria for SLE. Semin. Arthritis Rheum. 2019. 49(3S). S14-S17. doi: 10.1016/j.semarthrit.2019.09.009.
15. Hochberg M.C. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997. 40(9). 1725. doi: 10.1002/art.1780400928.
16. Gladman D.D., Ibañez D., Urowitz M.B. Systemic lupus erythematosus disease activity index 2000. J. Rheumatol. 2002. 29(2). 288-91.
17. Gladman D., Ginzler E., Goldsmith C. The deve–lopment and initial validation of the Systemic Lupus International Collaborating Clinics/American College of Rheumatology damage index for systemic lupus erythematosus. Arthritis Rheum. 1996. 39(3). 363-9. doi: 10.1002/art.1780390303.
18. Вороненко Ю.В., Москаленко В.Ф. Соціальна медицина та організація охорони здоров’я. Тернопіль: Укрмедкнига, 2000. С. 680.
19. Pavlov-Dolijanovic S., Damjanov N.S., Vujasinovic Stupar N.Z., Marcetic D.R., Sefik-Bukilica M.N., Petrovic R.R. Is there a difference in systemic lupus erythematosus with and without Raynaud’s phenomenon? Rheumatol. Int. 2013. 33(4). 859-65. doi:10.1007/s00296-012-2449-6.
20. Poh Y.J., Baptista B., D’Cruz D.P. Subcutaneous and intravenous belimumab in the treatment of systemic lupus erythematosus: a review of data on subcutaneous and intravenous administration. Expert Rev. Clin. Immunol. 2017. 13(10). 925-938. doi: 10.1080/1744666X.2017.1371592.

/24.jpg)
/25.jpg)