
Журнал «Боль. Суставы. Позвоночник» Том 13, №1, 2023
Вернуться к номеру
Деякі клінічні чинники виникнення асептичної нестабільності ендопротеза колінного суглоба
Авторы: Сулима О.М., Калашніков О.В., Підгаєцький В.М., Козак Р.А., Нізалов Т.В.
ДУ «Інститут травматології та ортопедії НАМН України», м. Київ, Україна
Рубрики: Ревматология, Травматология и ортопедия
Разделы: Клинические исследования
Версия для печати
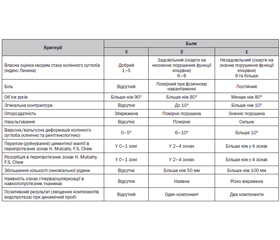
Актуальність. Проведення клінічних досліджень з визначення чинників виникнення асептичної нестабільності компонентів ендопротеза колінного суглоба є актуальним питанням сучасної ортопедії. Метою дослідження було визначення деяких клінічних чинників асептичної нестабільності компонентів ендопротеза колінного суглоба. Матеріали та методи. Проведено комплексні дослідження 285 пацієнтів, яким виконано первинне ендопротезування колінного суглоба в терміни з 2010 по 2021 рік, з них 85 осіб з клініко-рентгенологічними ознаками асептичної нестабільності компонентів ендопротеза колінного суглоба (АНКЕКС). 200 хворих становили контрольну групу, у якій ознак нестабільності АНКЕКС не спостерігали. Клінічні методи досліджень включали загальноклінічні, загальні та спеціальні ортопедичні методи вивчення локальних змін у колінному суглобі. До них відносили визначення індексу маси тіла (ІМТ), перевантаження колінного суглоба внаслідок умов праці, попередніх оперативних втручань та ранніх післяопераційних ускладнень первинного ендопротезування, наявності кутових деформацій у колінному суглобі. Для клінічної оцінки колінного суглоба хворих після тотального ендопротезування колінного суглоба користувались власною бальною оцінкою його стану. Результати. Визначено, що вірогідними чинниками розвитку нестабільності компонентів ендопротеза колінного суглоба є як ті, що безпосередньо пов’язані з пацієнтом (збільшення ІМТ, важкість умов праці, наявність оперативних втручань на колінному суглобі), так і пов’язані з помилками під час виконання первинного тотального ендопротезування (залишкові деформації колінного суглоба та ранні післяопераційні ускладнення). Висновки. Визначені чинники асептичної нестабільності колінного суглоба. Результати цього дослідження дозволять поліпшити діагностику та лікування асептичної нестабільності колінного суглоба.
Background. Conducting clinical studies to determine the factors determining the aseptic instability of knee joint endoprosthesis components is an urgent issue in modern orthopedics. The aim of the study was to determine some clinical factors of aseptic instability of knee joint endoprosthesis components. Materials and methods. Comprehensive research was conducted on 285 patients who underwent primary knee arthroplasty between 2010 and 2021, including 85 patients with clinical and radiological signs of aseptic instability of knee arthroplasty components (AIKAC). Also, 200 patients made up a control group with no signs of AIKAC instability observed. Clinical research methods included general, and special orthopedic methods of studying local changes in the knee joint. They included measurement of body mass index (BMI), overloading of the knee joint due to work, previous surgical interventions and early postoperative complications of primary arthroplasty, and presence of angular deformities in the knee joint. For the clinical assessment of the knee joint of patients after knee arthroplasty, we used our own point assessment of the state of the knee joint. Results. It was determined that significant factors for the development of instability of components of the knee joint endoprosthesis are both directly related to the patient (increase in BMI, difficult working conditions, the presence of operative interventions on the knee joint), and factors related to errors during the primary total arthroplasty (residual deformities of the knee joint and early postoperative complications). Conclusions. We determined important factors of aseptic instability of the knee joint in the patients after arthroplasty. Taking into account the results of this study will improve the diagnosis and treatment of aseptic instability of the knee joint.
ендопротез колінного суглоба; асептична нестабільність; клінічні чинники
knee arthroplasty; aseptic instability; clinical factors
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Agency for Healthcare Recearch and Quality. HCUP Databases. Healthcare Cost and Utilization Project (HCUP). 2008. January 9, 2009. Available at: http://www.hcup-us.ahrq.gov/nisoverview.jsp.
- Ong K.L., Lau E., Kurtz S.M., Manly M.T. Risk of subsequent revision after primary and revision total joint arthroplasty. Clin. Orthoped. Relat. Res. 2010. 468(11). 3070-3076. doi: 10.1007/s11999-010-1399-0.
- Bozic K.J., Durbhakula S., Berry D.J., Naessens J.M., Rappaport K., Miriam C., Khaled J.S., Rubash H.E. Diffe–rences in patient and procedure characteristics and hospital resource use in primary and revision total joint arthroplasty: multicenter study. J. Arthroplasty. 2005. 20(7). 17-25. doi: 10.1016/j.arth.2005.04.021.
- Loeser R.F., Goldrina S.R., Scanzello C.R., Goldring M.B. Osteoarthritis: A Disease of the Joint as an Organ. Arthritis Rheum. 2012. 64(6). 1697-1707. doi: 10.1002/art.34453.
- Barrack R.L., Hoffman G.J., Tejeiro W.V., CarpenterL.J. Jr. Surgeon work input and risk in primary versus revisiontotal joint arthroplasty J. Arthroplasty. 1995. 10. 281-286. doi: 10.1016/s0883-5403(05)80175-5.
- Ritter M.A., Carr K.D. Revision total joint arthroplasty: dose Medicare reimbursement justify time spent? Orthopedics. 1996. 19. 137-139. doi: 10.3928/0147-7447-19960201-08.
- Hebert C.K., Williams R.E. Cost of treating an infected total knee replacement. Clin. Orthop. 1996. 331. 140-145. doi: 10.1097/00003086-199610000-00019.
- Bozic K., Kurtz S., Lau E., Kevin Ong К., Chiu V., Vail T.P., Rubash H.E., Berry D.J. The epidemiology of revision total knee arthroplasty in the United States. Clin. Orthop. 2010. 468. 45-51. doi: 10.1007/s11999-009-0945-0.
- Clarke H.D., Scuderi G.R. Revision total knee arthroplasty: planning, management, controversies and surgical approaches. Instr. Course Lect. 2001. 50. 359-365. PMID: 11372334.
- Mulcahy H., Chew F.S. Current Concepts in Knee Replacement: Complications. American Journal of Roentgenology. 2014/ 202/ 76-86. doi: 10.2214/AJR.13.11308.
- Гайко Г.В., Осадчук Т.І., Заєць В.Б., Підгаєцький В.М., Сулима О.М., Калашніков О.В. Диференційний підхід до ендопротезування колінного суглоба у хворих на гонартроз залежно від тяжкості ураження. Вісник ортопедії, травматології та протезування. 2017. 2. 59-66.
- Lequesne M.G. The algofunctional indices for hip and knee osteoarthritis. J. Rheumat. 1997. 24. 779-781. PMID: 9101517.
- Лапач С.Н., Чубенко А.В., Бабич П.Н. Статистические методы в биологических исследованиях с использованием Excel. К.: Морион, 2000. 320 с.
- Мінцер О.П., Вороненко Ю.В., Власов В.В. Інформаційні технології в охороні здоров’я і практичній медицині [у 10 кн.]: Оброблення клінічних і експериментальних даних у медицині: Навч. посіб., кн. 5. К.: Вища школа, 2003. 350 с.
- Hofmann S., Seitlinger G., Djahani O., Pietsch M. The painful knee after TKA: a diagnostic algorithm for fai–lure analysis. Knee Surg. Sports Traumatol. Arthrosc. 2011. 19(9). 1442-1452. doi: 10.1007/s00167-011-1634-6.
- Hawker G.A., Mian S., Kendzerska T., French M. Measures of adult pain. Arthritis Care Res. (Hoboken). 2011. 63 (11). 240-52. doi: 10.1002/acr.20543.
- Kornilov N., Lindberg M.F., Gay C., Saraev A., Kuliaba T., Rosseland L.A. et al. Higher physical activity and lower pain levels before surgery predict non-improvement of knee pain 1 year after TKA. Knee Surg. Sport Traumatol. Arthrosc. 2018. 26(6). 1698-1708. doi: 10.1007/s00167-017-4713-5.
- Insall J., Salvati E. Patella position in the normal knee joint. Radiology. 1971. 101(1). 101-104. doi: 10.1148/101.1.101.
- Blackburne J.S, Peel T.E. A new method of measu–ring patellar height. J. Bone Joint Surg. Br. 1977. 59(2). 241-242. doi: 10.1302/0301-620X.59B2.873986.
- Behrend H., Graulich T., Gerlach R., Spross C., Ladurner A. Blackburne–Peel ratio predicts patients’ outcomes after total knee arthroplasty. Knee Surg. Sport Traumatol. Arthrosc. 2019. 27(5). 1562-1569. doi: 10.1007/s00167-018-5016-1.
- Berger R.A., Crossett L.S., Jacobs J.J., Rubash H.E. Malrotation causing patellofemoral complications after total knee arthroplasty. Clin. Orthop. Relat. Res. 1998. (356). 144-153. doi: 10.1097/00003086-199811000-00021.
- Berger R.A., Crossett L.S. Determining the rotation of thefemoral and tibial components in total knee arthroplasty: A computer tomography technique. Oper. Tech. Orthop. 1998. 8(3). 128-133. doi: 10.1016/S1048-6666(98)80022-0.
- Seil R., Pape D. Causes of failure and etiology of painful primary total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2011. 19(9). 1418-1432. doi: 10.1007/s00167-011-1631-9.
- Momoli A., Giaretta S., Modena M., Micheloni G.M. The painful knee after total knee arthroplasty: evaluation and management. Acta Biomed. 2017. 88(2S). 60-67. doi: 10.23750/abm.v88i2 -S.6515.
- Merchant A.C., Mercer R.L., Jacobsen R.H., Cool C.R. Roentgenographic analysis of patellofemoral congruence. J. Bone Joint Surg. Am. 1974. 56(7). 1391-1396. PMID: 4433362.
- Жиженкова Т.В., Даниляк В.В., Ключевский В.В., Ключевский В.В. Оценка нестабильности надколенника после тотального эндопротезирования коленного сустава. Травматология и ортопедия России. 2015. (2). 24-31. doi: 10.21823/2311-2905-2015-0-2-24-31.
- Tahmasebi M.N., Amjad G.G., Bashti K. Total Knee Arthroplasty in Severe Unstable Knee: Case Report and Literature Review. Arch. Bone Jt Surg. 2017. 5(1). 58-62. PMID: 28271089.
- Fang D.M., Ritter M.A., Davis K.E. Coronal alignment in total knee arthroplasty: just how important is it? J. Arthroplasty. 2009. 23. 39-43. doi: 10.1016/j.arth.2009.04.034.
- Gupta S.K., Chu A., Ranawat A.S., Shamin J. Osteolysis after total knee arthroplasty. J. Arthroplasty. 2007. 22(6). 787-799. doi: 10.1016/j.arth.2007.05.041.
- Schmalzried T.P., Shepherd E.F., Dorey F.J. The John Charnley Award. Wear is a function of use, not time. Clin. Orthoped. Relat. Res. 2000. 12(381). 36-46. doi: 10.1097/00003086-200012000-00005.