
Журнал "Гастроэнтерология" Том 58, №1, 2024
Вернуться к номеру
Роль ендоскопічного ультразвукового дослідження в оцінці неспроможності фізіологічної кардії при діагностиці гриж стравохідного отвору діафрагми
Авторы: Шевченко Б.Ф., Бабій О.М., Пролом Н.В., Тітова М.В., Тарабаров С.О., Ущіна С.В.
ДУ «Інститут гастроентерології НАМН України», м. Дніпро, Україна
Рубрики: Гастроэнтерология
Разделы: Клинические исследования
Версия для печати
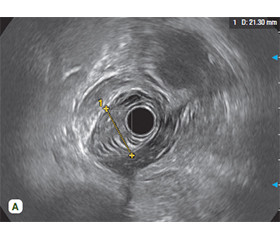
Мета дослідження: визначити роль ендоскопічного ультразвукового дослідження в оцінці неспроможності фізіологічної кардії при діагностиці гриж стравохідного отвору діафрагми (ГСОД). Матеріали та методи. У відділі хірургії органів травлення Державної установи «Інститут гастроентерології НАМН України» в 2023 р. згідно із завданнями роботи проведено дослідження у 33 пацієнтів з ГСОД, зокрема: аксіальні ГСОД (n = 21 (63,6 %)) — І тип; параезофагеальні ГСОД (n = 12 (36,4 %)) — ІІ тип (код за МКХ-10 — К 44), та у 20 практично здорових осіб (контрольна група). Усім пацієнтам проводили рентгенологічне та ендоскопічне дослідження стравоходу, шлунка, дванадцятипалої кишки, ендоскопічну ультрасонографію (ЕУС). Результати. Усім 33 (100,0 %) пацієнтам для підтвердження діагнозу виконано рентгенологічне дослідження, для виявлення змін слизової оболонки стравоходу — ендоскопічне дослідження. У 31 (93,9 %) пацієнта виконано ЕУС. При дослідженні за допомогою ЕУС-сканування визначали товщину стінки стравоходу, що дало змогу визначити стан структур фізіологічної кардії при ГСОД: зміщення частини шлунка над діафрагмою, розміщення стравохідно-шлункового переходу відносно ніжок СОД та відносно один одного; відстань між ніжками СОД та їх довжину, площу СОД та площу поперечного перерізу ГСОД (грижового мішка). Отримані при ЕУС дані вплинули на вибір способу хірургічної корекції фізіологічної кардії при ГСОД. Висновки. Таким чином, при ГСОД ЕУС-дослідження дає можливість оцінити патологічні зміни основних структур неспроможної фізіологічної кардії, поліпшити діагностику у визначенні типів ГСОД, розташування стравохідно-шлункового переходу з визначенням розмірів СОД, відстані між ніжками фізіологічної кардії, локалізацію та поперечний переріз грижового мішка, що вплинуло на вибір способу хірургічної корекції фізіологічної кардії при ГСОД.
Background. The aim of the study: to determine the role of endoscopic ultrasound (EUS) in assessing the failure of the physiological cardia in the diagnosis of hiatal hernias (HH). Materials and methods. At the Department of Digestive Surgery of the State Institution “Institute of Gastroenterology of the National Academy of Medical Sciences of Ukraine” in 2023, we have performed surgical treatment of 33 patients with HH: axial HH were diagnosed in 21 (63.6 %) cases (I type), paraesophageal HH — in 12 (36.4 %) patients (II type) (ICD-10 code is K44). Control group included 20 practically healthy people. Results. All patients underwent an X-ray and endoscopic examination of the esophagus, stomach, duodenum, and EUS. All 33 (100.0 %) patients underwent an X-ray to confirm the diagnosis and an endoscopic examination to detect changes in the esophageal mucosa. EUS was performed in 31 (93.9 %) patients. The thickness of the esophageal wall was assessed using EUS, which made it possible to determine the state of the structures of the physiological cardia in HH: the displacement of part of the stomach above the diaphragm, location of the gastroesophageal junction relative to the legs of the diaphragm and relative to each other; the distance between the legs of the diaphragm (area of the HH) and their length; the cross-sectional area of the HH (hernial sac). The data obtained during EUS influenced the choice of the method for surgical correction of the physiological cardia with HH. Conclusions. Thus, with HH, EUS makes it possible to evaluate pathological changes of the main structures in the failure of the physiological cardia, to improve diagnosis for the types of HH, the location of the gastroesophageal junction, with determination of dimensions of the esophageal hiatus, the distance between the legs of the physiological cardia, localization and cross-section of the hernial sac, which influenced the choice of the surgery for physiological cardia in HH.
неспроможність фізіологічної кардії; грижа стравохідного отвору діафрагми; ендосонографія; еластометрія
insufficiency of physiological cardia; hiatal hernia; endosonography; elastometry
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Степанов Ю.М., Пролом Н.В. Діагностика і хірургічне лікування гриж стравохідного отвору діафрагми. Київ: Видавець Заславський О.Ю., 2021. 254 с.
- Nurczyk K., Corpo M.D., Patti M.G. Hiatal hernia. Benign Eso–phageal Disease: Modern Surgical approaches and Techniques. Springer. 2021. № 3. P. 59-71. https://doi.org/10.1007/978-3-030-51489-1.
- Cesario S., Scida S., Miraglia C. et al. Diagnosis of GERD in typical and atypical manifestations. Acta Biomed. 2018. № 89(8). Р. 33-39. https://doi.org/10.23750/abm.v89i8-S.7963.
- Dias P.N.G., Neto R.M.L., Fernando A.M. et al. Psychiatric symptoms and the upper esophageal sphincter. Surg. Gastroenterol. Oncol. 2020. № 3(25). Р. 121-124. DOI: 10.21614/sgo-25-3-121.
- Andolfi C., Plana A., Furno S., Fisichella P.M. Paraesophageal Hernia and Reflux Prevention: Is One Fundoplication Better than the Other? World J Surg. 2017. № 4(10). P. 2573-2582. doi: 10.1007/s00268-017-4062-z.
- Ghisa M., Della Coletta M., Barbuscio I., Marabotto E., Barberio B., Frazzoni M. et al. Updates in the field of non-esophageal gastroesophageal reflux disorder. Expert Rev Gastroenterol Hepatol. 2019. № 13. P. 827-838. DOI: 10.1080/17474124.2019.1645593.
- Rajkomar K., Berney C.R. Large hiatus hernia: time for a paradigm shift? BMC Surg. 2022. № 264. 22 р. https://doi.org/10.1186/s12893-022-01705-w.
- Turner B., Helm M., Hetzel E., Schumm M., Gould J.C. The relationship between gastroesophageal junction integrity and sympto–matic fundoplication outcomes. Surg Endosc. 2020. № 3 (34). P. 1387-1392. doi: 10.1007/s00464-019-06921-9. Epub 2019 Jun 18. PMID: 31214803.
- Kanani Z., Gould J.C. Laparoscopic fundoplication for refractory GERD: a procedure worth repeating if needed. Surg Endosc. 2021. № 35. P. 298-302. https://doi.org/10.1007/s00464-020-07396-9.
- Neto R.M.L., Herbella F.A.M., Zugman A. et al. Minor psychiatric disorders and objective diagnosis of gastroesophageal reflux disease. Surg Endosc. 2019. № 33. Р. 4116-4121. https://doi.org/10.1007/s00464-019-06716-y.
- Siegal S.R., Dolan J.P., Hunter J.G. Modern diagnosis and treatment of hiatal hernias. Langenbecks Arch Surg. 2017. V. 402. № 8. P. 1145-1151. doi: 10.1007/s00423-017-1606-5. Epub 2017 Aug 21. PMID: 28828685.
- Hocke M., Braden B., Jenssen C., Dietrich C.F. et al. Present status and perspectives of endosonography 2017 in gastroenterology. Korean J Intern Med. 2018. № 33(1). P. 36-63. doi: 10.3904/kjim.2017.212.
- Iglesias-Garcia J., de la Iglesia-Garcia D., Lariño-Noia J., Dominguez-Muñoz J.E. Endoscopic Ultrasound (EUS) Guided Elastography. Diagnostics. 2023. № 13(10). P. 1686. https://doi.org/10.3390/diagnostics13101686.
- Candoli P., Ceron L., Trisolini R. et al. Competence in endosonographic techniques. Panminerva Med. 2019. № 61(3). P. 249-279. doi: 10.23736/S0031-0808.18.03570-X.
- Степанов Ю.М., Пролом Н.В., Коненко І.С., Тарабаров С.О., Недзвецька Н.В. Ендоскопічна ультразвукова сонографія в діагностиці патології шлунково-кишкового тракту. Гастроентерологія. 2021. Т. 55. № 3. С. 62-68. DOI: https://doi.org/10.22141/2308-2097.55.3.2021.241590.
- Dhar J., Samanta J. The expanding role of endoscopic ultrasound elastography. Clin J Gastroenterol. 2022. № 15(5). Р. 841-858. doi: 10.1007/s12328-022-01662-0. PMID: 35789474.
- Cui X.W., Chang J.M., Kan Q.C., Chiorean L., Ignee A., Dietrich C.F. Endoscopic ultrasound elastography: Current status and future perspectives. World J Gastroenterol. 2015. № 21(47). Р. 13212-13224. PMID: 26715804. DOI: 10.3748/wjg.v21.i47.13212.
- Seicean A., Mosteanu O., Seicean R. Maximizing the endosonography: The role of contrast harmonics, elastography and confocal endomicroscopy. World J Gastroenterol. 2017. № 23(1). Р. 25-41. doi: 10.3748/wjg.v23.i1.25.
- Pih G.Y., Kim D.H. Endoscopic Ultrasound-Guided Fine Needle Aspiration and Biopsy in Gastrointestinal Subepithelial Tumors. Clin Endosc. 2019. № 52(4). Р. 314-320. doi: 10.5946/ce.2019.100.
- Kitano M., Yoshida T., Itonaga M. et al. Impact of endoscopic ultrasonography on diagnosis of pancreatic cancer. Gastroenterol. 2019. № 54(1). Р. 19-32. doi: 10.1007/s00535-018-1519-2.