Резюме
Мета роботи: вивчити характеристику факторів серцево-судинного ризику (ССР), структуру та ефективність терапії в пацієнтів з артеріальною гіпертензією (АГ) на тлі подвійної комбінації антигіпертензивних препаратів. Матеріали та методи. Багатоцентрове дослідження за участі 1616 пацієнтів з АГ, які приймали подвійну комбіновану антигіпертензивну терапію. Вивчали фактори ССР (статус куріння, споживання алкоголю, фізичну активність, наявність обтяженого сімейного серцево-судинного анамнезу), супутні серцево-судинні захворювання, порушення вуглеводного обміну, визначали індекс маси тіла, оцінювали поточну антигіпертензивну терапію та її ефективність за даними офісних вимірювань артеріального тиску. Результати. Пацієнти з АГ характеризувалися значною поширеністю ожиріння (38,6 %), куріння (27,9 %), недостатньої фізичної активності (31,2 %). Суттєво вищий відсоток куріння та вживання алкоголю був зареєстрований серед чоловіків, натомість нижчий рівень фізичної активності — серед жінок. Супутній цукровий діабет 2-го типу був наявним практично у чверті пацієнтів, перенесений інсульт/ТІА — у 8,7 %, інфаркт міокарда/реваскуляризація — у 8,3 %. При цьому статинотерапію отримували 53,2 % обстежених, антитромбоцитарні препарати — 64,7 %. Висновки. Ефективність подвійної антигіпертензивної теарпії становила 15,6 %. У структурі антигіпертензивної терапії домінували комбінації іАПФ з тіазидним/тіазидоподібним діуретиком — 42,7 %; іАПФ з БКК отримували 6,4 %. БРА частіше призначалися в комбінації з діуретиком — 31,4 %, з БКК — 9,4 %. Поміж інших комбінацій частіше використовували іАПФ з бета-блокатором — 9 %. У призначеннях переважали фіксовані комбінації антигіпертензивних препаратів, їх частка сягала 84,5 %.
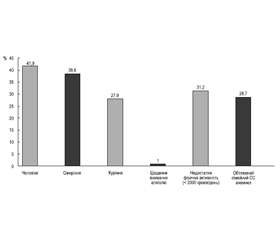
Background. The purpose was to study the characteristics of cardiovascular risk factors, the structure, and the effectiveness of treatment in hypertensive patients using a dual combination of antihypertensive drugs. Materials and methods. A multicenter study enrolled 1616 hypertensive patients who received dual combination antihypertensive therapy. Cardiovascular risk factors (smoking status, alcohol consumption, physical activity, family history of cardiovascular disease), concomitant cardiovascular diseases, carbohydrate metabolism disorders were studied, as well as body mass index, current antihypertensive therapy and its effectiveness based on office blood pressure measurements. Results. Hypertensive patients were characterized by a significant prevalence of obesity (38.6 %), smoking (27.9 %), and insufficient physical activity (31.2 %). A significantly higher percentage of smoking and alcohol consumption was registered among men, while the level of physical activity was lower among women. Concomitant type 2 diabetes was present in almost a quarter of patients, stroke/transient ischemic attack — in 8.7 %, myocardial infarction/revascularization — in 8.3 %. At the same time, 53.2 % of the patients received statin therapy, and 64.7 % took antiplatelet drugs. Conclusions. The effectiveness of dual antihypertensive therapy was 15.6 %. Combinations of angiotensin-converting enzyme (ACE) inhibitors with a thiazide/thiazide-like diuretic dominated in the structure of antihypertensive therapy — 42.7 %, ACE inhibitors with calcium channel blockers were administered to 6.4 % of patients. Angiotensin II receptor blockers were more often prescribed in combination with a diuretic — 31.4 %, calcium channel blockers — 9.4 %. Among other combinations, ACE inhibitors with a beta-blocker were used more often (9 %). Fixed combinations of antihypertensive drugs were prescribed in 84.5 % of cases.
Список литературы
1. NCD Risk Factor Collaboration (NCD-RisC) (2021). Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet (London, England), 398(10304), 957-980. https://doi.org/10.1016/S0140-6736(21)01330-1.
2. Kario, K., Okura, A., Hoshide, S., & Mogi, M. (2024). The WHO Global report 2023 on hypertension warning the emerging hypertension burden in globe and its treatment strategy. Hypertension Research: official journal of the Japanese Society of Hypertension, 47(5), 1099-1102. https://doi.org/10.1038/s41440-024-01622-w.
3. van Oort, S., Beulens, J.W.J., van Ballegooijen, A.J., Grobbee, D.E., & Larsson, S.C. (2020). Association of Cardiovascular Risk Factors and Lifestyle Behaviors With Hypertension: A Mendelian Randomization Study. Hypertension (Dallas, Tex.: 1979), 76(6), 1971-1979. https://doi.org/10.1161/HYPERTENSIONAHA.120.15761.
4. Global Cardiovascular Risk Consortium, Magnussen, C., Ojeda, F.M., Leong, D.P., Alegre-Diaz, J., Amouyel, P., Aviles-Santa, L., … Blankenberg, S. (2023). Global Effect of Modifiable Risk Factors on Cardiovascular Disease and Mortality. The New England Journal оf Medicine, 389(14), 1273-1285. https://doi.org/10.1056/NEJMoa2206916.
5. Coca, A., Borghi, C., Stergiou, G.S., Khan, I., Koumas, A., Blacher, J., Abdel-Moneim, M. (2024). Estimated impact of guidelines-based initiation of dual antihypertensive therapy on long-term cardiovascular outcomes in 1.1 million individuals, European Heart Journal — Cardiovascular Pharmacotherapy, pvae048. https://doi.org/10.1093/ehjcvp/pvae048.
6. Brant, L.C.C., Passaglia, L.G., Pinto-Filho, M.M., de Castilho, F.M., Ribeiro, A.L.P., & Nascimento, B.R. (2022). The Burden of Resistant Hypertension Across the World. Current Hypertension Reports, 24(3), 55-66. https://doi.org/10.1007/s11906-022-01173-w.
7. Manta, E., Thomopoulos, C., Kariori, M., Polyzos, D., Mihas, C., Konstantinidis, D., Farmakis, D., Mancia, G., & Tsioufis, K. (2024). Revisiting Cardiovascular Benefits of Blood Pressure Reduction in Primary and Secondary Prevention: Focus on Targets and Residual Risk — A Systematic Review and Meta-Analysis. Hypertension (Dallas, Tex.: 1979), 81(5), 1076-1086. https://doi.org/10.1161/HYPERTENSIONAHA.123.22610.
8. Gnanenthiran, S.R., Wang, N., Di Tanna, G.L., Salam, A., Webster, R., de Silva, H.A., … Rodgers, A., & TRIUMPH Study Group (2022). Association of Low-Dose Triple Combination Therapy vs Usual Care With Time at Target Blood Pressure: A Secondary Analysis of the TRIUMPH Randomized Clinical Trial. JAMA Сardiology, 7(6), 645-650. https://doi.org/10.1001/jamacardio.2022.0471.
9. Mancia, G., Kreutz, R., Brunstrm, M., Burnier, M., Grassi, G., Januszewicz, A., … Kjeldsen, S.E. (2023). 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension: Endorsed by the International Society of Hypertension (ISH) and the European Renal Association (ERA). Journal of Hypertension, 41(12), 1874-2071. https://doi.org/10.1097/HJH.0000000000003480.
10. Stergiou, G.S., Palatini, P., Parati, G., O’Brien, E., Januszewicz, A., Lurbe, E., Persu, A., Mancia, G., Kreutz, R., & European Society of Hypertension Council and the European Society of Hypertension Working Group on Blood Pressure Monitoring and Cardiovascular Variability (2021). 2021 European Society of Hypertension practice guidelines for office and out-of-office blood pressure measurement. Journal of Hypertension, 39(7), 1293-1302. https://doi.org/10.1097/HJH.0000000000002843.
11. Jawad, M., Vamos, E.P., Najim, M., Roberts, B., & Millett, C. (2019). Impact of armed conflict on cardiovascular disease risk: a systematic review. Heart (British Cardiac Society), 105(18), 1388-1394. https://doi.org/10.1136/heartjnl-2018-314459.
12. GBD 2017 Risk Factor Collaborators (2018). Global, regional, and national comparative risk assessment of 84 beha–vioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet (London, England), 392(10159), 1923-1994. https://doi.org/10.1016/S0140-6736(18)32225-6.
13. Mishchenko L., on behalf of the group of investigators (2019). Efficiency of monotherapy for blood pressure control: results of Ukrainian MAHNAT study. UJC, 26(5), 11-20. doi: 10.31928/10.31928/1608-635X-2019.5.1120.
14. Hayashi, T., Tsumura, K., Suematsu, C., Okada, K., Fujii, S., & Endo, G. (1999). Walking to work and the risk for hypertension in men: the Osaka Health Survey. Annals of Internal Medicine, 131(1), 21-26. https://doi.org/10.7326/0003-4819-131-1-199907060-00005.
15. Hayes, P., Ferrara, A., Keating, A., McKnight, K., O’Regan, A. (2022). Physical Activity and Hypertension. Rev. Cardiovasc. Med., 23(9), 302. https://doi.org/10.31083/j.rcm2309302.
16. Mills, K.T., Stefanescu, A., & He, J. (2020). The global epidemiology of hypertension. Nature Reviews. Nephrology, 16(4), 223-237. https://doi.org/10.1038/s41581-019-0244-2.
17. Gender-Related Factors in Medication Adherence for Metabolic and Cardiovascular Health. Metabolites, 13(10), 1087. https://doi.org/10.3390/metabo13101087.
18. Tajeu, G.S., Kent, S.T., Kronish, I.M., Huang, L., Krousel-Wood, M., Bress, A. P., Shimbo, D., & Muntner, P. (2016). Trends in Antihypertensive Medication Discontinuation and Low Adherence Among Medicare Beneficiaries Initiating Treatment From 2007 to 2012. Hypertension (Dallas, Tex.: 1979), 68(3), 565-575. https://doi.org/10.1161/HYPERTENSIONAHA.116.07720.