
Журнал «» Том 18, №1, 2025
Вернуться к номеру
Варіанти вторинних гіпертензій серед пацієнтів із резистентною артеріальною гіпертензією в умовах стаціонарного відділення
Авторы: Рековець О.Л. (1), Сіренко Ю.М. (2), Мальчевська Т.Й. (3)
(1) - ДУ «ННЦ «Інститут кардіології, клінічної та регенеративної медицини імені академіка М.Д. Стражеска НАМН України», м. Київ, Україна
(2) - Національний університет охорони здоров’я України ім. П.Л. Шупика, м. Київ, Україна
(3) - Національний медичний університет імені О.О. Богомольця, м. Київ, Україна
Рубрики: Кардиология
Разделы: Клинические исследования
Версия для печати
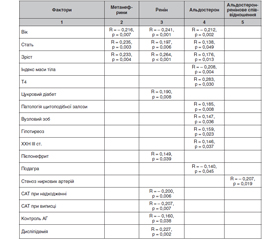
Актуальність. На сьогодні згідно з новими рекомендаціями 2024 року ESC з підвищеного АТ та гіпертензії велика увага приділяється виявленню вторинних форм артеріальної гіпертензії (АГ) як однієї з причин резистентної АГ. Тому згідно з рекомендаціями усім пацієнтам старше ніж 40 років з доведеною гіпертензією рекомендовано визначення ренін-альдостеронового співвідношення для пошуку гіперальдостеронізму. Метою нашого дослідження було виявлення частки пацієнтів із вторинними формами АГ серед хворих із ймовірно резистентною АГ. Матеріали та методи. У дослідження було включено 1146 пацієнтів із ймовірно резистентною АГ, які приймали 3 та більше антигіпертензивні препарати. Біохімічне дослідження крові виконували на автоматичному біохімічному аналізаторі «А25» (BioSystems, Іспанія) в лабораторії ДУ «ННЦ «Інститут кардіології, клінічної та регенеративної медицини ім. акад. М.Д. Стражеска НАМН України». Розраховували ШКФ з використанням формули CKD-EPI. Визначали рівень калію, натрію, креатиніну, глюкози, ліпідного спектра крові. Рівень реніну, альдостерону крові, ренін/альдостеронове співвідношення, кортизол крові та метанефрини в добовій сечі, гормони щитоподібної залози — Т3, Т4, ТТГ — визначали в лабораторії. Результати. Обстежено 1146 пацієнтів із ймовірно резистентною АГ, що приймали 3 та більше антигіпертензивні препарати. Жінок порівняно з чоловіками було більше — 62,7 %. 39,3 % пацієнтів мали ожиріння. Дисліпідемія виявлена у 64,8 % пацієнтів. Цукровий діабет II типу — у 16,6 %. У 88,5 % пацієнтів була виявлена есенціальна АГ. Порушення мозкового кровообігу в анамнезі було у 15,8 % пацієнтів, переважав ішемічний інсульт — 12,8 %. 51,4 % пацієнтів приймали 3 препарати. Решта пацієнтів — 48,6 % — приймали 4–6 препаратів: серед них переважна більшість приймала 4 препарати (37,1 %), 9,1 % приймали 5 препаратів та 2,4 % — 6 препаратів. У 11,52 % пацієнтів (n = 132) була виявлена вторинна АГ. Серед них аденома наднирників виявлена в 3,05 % пацієнтів (n = 35) серед усієї групи пацієнтів та 26,51 % серед пацієнтів із вторинною АГ. Порушення функції щитоподібної залози — у 3,49 % пацієнтів (n = 40) серед усієї групи та 30,30 % серед пацієнтів із вторинною АГ. Стеноз ниркових артерій виявлено у 3,05 % пацієнтів (n = 35) серед всієї групи та 26,51 % серед пацієнтів із вторинною АГ. Аномалії ниркових судин виявлені в 1,00 % пацієнтів (n = 11) серед усієї групи та 8,33 % серед пацієнтів із вторинною АГ. Фібромускулярна дисплазія виявлена у 0,35 % пацієнтів (n = 4) серед усієї групи та 3,03 % серед пацієнтів із вторинною АГ. Стентування ниркових артерій було проведено у 0,35 % пацієнтів (n = 4) серед усієї групи та 3,03 % серед пацієнтів із вторинною АГ. Аденома гіпофіза спостерігалась у 0,26 % пацієнтів (n = 3) серед усієї групи та 2,27 % серед пацієнтів із вторинною АГ. При аналізі кореляційних зв’язків ми виявили, що рівень альдостерону був прямо пов’язаний із патологією щитоподібної залози, наявністю вузлового зоба та гіпотиреозом. При пієлонефриті був підвищений рівень реніну крові, а при подагрі був більш низький рівень альдостерону крові. Стеноз ниркових артерій зворотно корелював із ренін-альдостероновим співвідношенням. Рівень офісного САТ зворотно корелював із рівнем реніну крові, при більш низькому рівні реніну крові був вищим рівень офісного САТ як при надходженні в стаціонар, так і при виписці, і, як наслідок, був гірший контроль АТ. Висновки. Вторинну артеріальну гіпертензію виявлено у 11,52 % пацієнтів із резистентною АГ, серед них найчастіше виявлялись аденома наднирникових залоз та порушення функції щитоподібної залози — у 56,81 %. Низький рівень реніну плазми крові асоціювався з незниженням офісного АТ.
Background. Today, according to the new 2024 ESC guidelines on high blood pressure and hypertension, much attention is paid to the detection of secondary forms of hypertension as one of the causes of resistant hypertension. Therefore, according to the recommendations, all patients over 40 years of age with proven hypertension are recommended to determine the renin-aldosterone ratio to search for hyperaldosteronism. The purpose of our study was to identify patients with secondary forms of hypertension among those with probably resistant hypertension. Materials and methods. The study included 1146 patients with probably resistant hypertension who took 3 or more antihypertensive drugs. Biochemical analysis of blood was performed on an A25 automatic analyzer (BioSystems, Spain) in the laboratory of the National Scientific Center “M.D. Strazhesko Institute of Cardiology, Clinical and Regeneration Medicine of NAMSU”. The glomerular filtration rate was calculated using the CKD-EPI formula. The levels of potassium, sodium, creatinine, glucose, blood lipids were determined. The content of renin, blood aldosterone, renin-aldosterone ratio, blood cortisol and metanephrine in daily urine, thyroid hormones (T3, T4, thyroid-stimulating hormone) were assessed in the laboratory. Results. 1146 patients with probably resistant hypertension who took 3 or more antihypertensive drugs were examined. There were more women than men — 62.7 %. Obesity was found in 39.3 % of patients, dyslipidemia — in 64.8 %, type II diabetes — in 16.6 %. Essential hypertension was detected in 88.5 % of cases. 15.8 % of patients had a history of cerebral circulation disorders, with ischemic stroke prevailing in 12.8 % of cases. 51.4 % of participants took 3 drugs. The rest, 48.6 %, took 4–6 drugs: among them, the vast majority, namely 37.1 %, took 4 drugs, 9.1 % took 5 drugs, and 2.4 % — six drugs. Secondary hypertension was detected in 11.52 % (n = 132) of cases. Adrenal adenoma was found in 3.05 % (n = 35) of all participants and 26.51 % of patients with secondary hypertension. Thyroid dysfunction was detected in 3.49 % (n = 40) of all participants and 30.30 % of patients with secondary hypertension. Renal artery stenosis was found in 3.05 % (n = 35) of all participants and 26.51 % of patients with secondary hypertension. Abnormalities of renal vessels occurred in 1.00 % (n = 11) of all participants and 8.33 % of patients with secondary hypertension. Fibromuscular dysplasia was found in 0.35 % (n = 4) of all participants and 3.03 % of patients with secondary hypertension. Renal artery stenting was performed in 0.35 % (n = 4) of all participants and 3.03 % of patients with secondary hypertension. Pituitary adenoma was observed in 0.26 % (n = 3) of all participants and 2.27 % of patients with secondary hypertension. When analyzing the correlations, we found that the aldosterone level was directly related to the thyroid pathology, the presence of nodular goiter, and hypothyroidism. In pyelonephritis, the blood renin was increased, and in gout, the blood aldosterone was lower. Renal artery stenosis inversely correlated with the renin-aldosterone ratio. The level of office systolic blood pressure inversely correlated with the content of blood renin; with a lower blood renin, office systolic blood pressure was higher both at admission to the hospital and at discharge, and as a result, blood pressure control was worse. Conclusions. Secondary hypertension was detected in 11.52 % of patients with resistant hypertension; adrenal adenoma and thyroid dysfunction were most often detected in them — 56.81 % of cases. Low level of plasma renin was associated with no decrease in office blood pressure.
артеріальна гіпертензія; вторинна артеріальна гіпертензія; ренін; альдостерон; метанефрини сечі; кортизол; прихильність до терапії; резистентна артеріальна гіпертензія; рефрактерна артеріальна гіпертензія
hypertension; secondary hypertension; renin; aldosterone; urinary metanephrines; cortisol; adherence to therapy; resistant hypertension; refractory hypertension