
Журнал «Здоровье ребенка» 2 (61) 2015
Вернуться к номеру
Complicated pneumococcal pneumonia in a child: case report.
Авторы: Kurochkin M.Yu., Davydova A.G., Kapusta V.N., Lyaturinskaya O.V., Skalozubov M.A., Kharitonov V.I., Bakhtina E.V., Zhmykhova S.A., Gorodkova Yu.V.
Zaporozhye State Medical University, Zaporozhye City Pediatric Multidiscipline Hospital #5, Ukraine
Рубрики: Педиатрия/Неонатология
Разделы: Клинические исследования
Версия для печати
Ключевые слова
pneumonia, pneumococcus, thoracoscopy, plasmapheresis.
Pneumococcal etiology diseases are an actual problem of practical public health because of the leading role Streptococcus pneumoniae in the structure of respiratory infections. Another problem associated with pneumococcal infection is the increase in bacterial resistance to antibiotics, including penicillins, III generation cephalosporins, macrolides, tetracyclines, and quinolones.
Despite the fact that the pneumococcus is the most common causative agent of lobar pneumonia in children, treatment of this disease remains difficult, course of the disease is heavy, and the outcome may be unpredictable, as the following case shows.
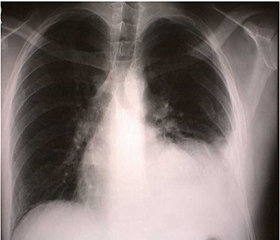
Patient N., an 8 years old girl, was admitted to the Pediatric Intensive Care Unit (PICU) in a grave condition with a diagnosis of right-sided lobar pneumonia complicated by exudative purulent pleurisy. On the second day, despite ongoing therapy, radiological investigation marked negative dynamics due to increased volume of lung infiltration, the destructive process in the right lung and the appearance of an infiltrate in the left lung. The results of bacteriological examinations of blood, pleural effusion and oropharynx revealed massive growth of Streptococcus pneumoniae. The diagnosis: Septicemia (Str.pneumoniae). Community-acquired pneumonia bilateral polysegmental: total destructive right-sided pleuropneumonia, focal left-sided (S10). Disseminated intravascular coagulation 1 degree, respiratory failure II degree.
From anamnesis, it is known that the girl had previously received whole complex of pneumococcal vaccination in Canada.
From the first day in PICU a child has got antibiotic combinations - meropenem with vancomycin with the change to levofloxacin and ceftriaxone/sulbactam, then to linezolid with amikacinum. In addition, discrete plasmapheresis was undertaken twice, and then immunotherapy with intravenous immunoglobulin was conducted. Infusion therapy in the mode of detoxification, nitrates and anticoagulants were administered. Improved sanitation with video assisted bronchoscopy, pleural cavity drainage by Byulau with the introduction of enzyme preparations into the pleural cavity was made.
Despite ongoing therapy desired positive dynamics were observed, particularly shortness of breath up to 70 breaths per minute and fever persisted, intoxication index (leukocyte index of intoxication by the Calf-Caliph formula, the nuclear index index by Dastayants, index of leukocytes shift by Lyubimova, the level of medium molecular peptides) met grave condition.
Due to the ineffectiveness of conservative therapy was concluded that the need for surgical sanitation the source of infection. On the eighth day of child’s stay in the PICU video assisted thoracoscopy was made. Fibrin scurf of the armor-clad density was found on the middle and lower lobes of the right lung, which was partially removed; pleural cavity drainages were administered.
The next day was marked by positive laboratory dynamics (indices of intoxication corresponded with moderate intoxication state, decreased almost twice). On the ninth day the third session of the discrete plasmapheresis was held, after which there was a clear positive trend both laboratory and clinically through shortness of breath regression, fever reducing, and the girl felt better.
The repeated bacteriological examination of the pleural cavity content and blood didn’t detect microorganisms growth. X-rays of the chest showed a positive trend of the pneumonic process, however, it revealed a right-sided fibrothorax. Availability of fibrothorax was also confirmed by computer tomography of the chest.
This case suggests that the main directions of the pneumococcal etiology destructive pneumonia therapy, besides antibiotic combinations based on the principle of de-escalation, are also a timely active surgical tactics in combination with extracorporeal methods of detoxification.